

Adrenal Incidentaloma
- PMID: 32266384
- PMCID: PMC7431180
- DOI: 10.1210/endrev/bnaa008
Adrenal Incidentaloma
Abstract
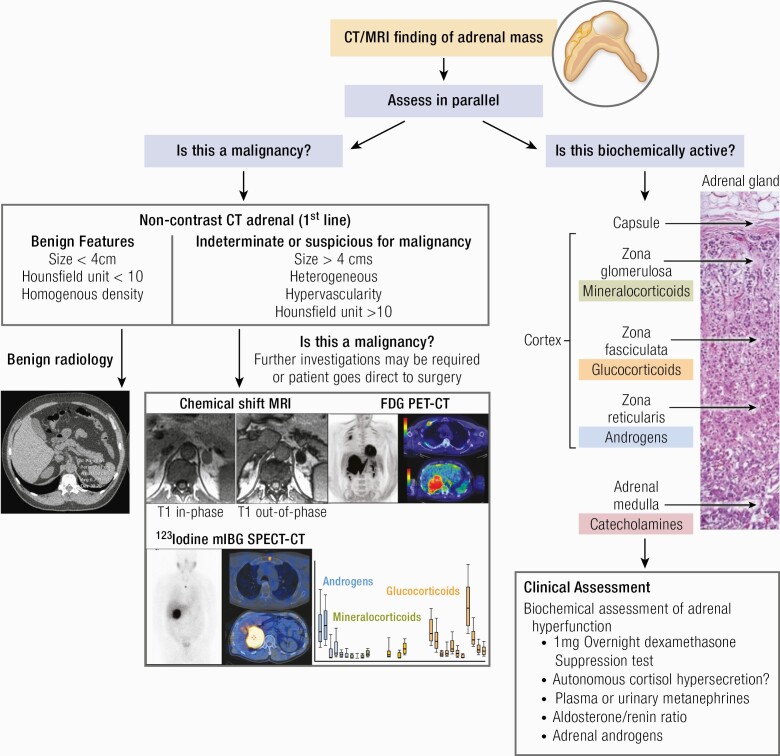
An adrenal incidentaloma is now established as a common endocrine diagnosis that requires a multidisciplinary approach for effective management. The majority of patients can be reassured and discharged, but a personalized approach based upon image analysis, endocrine workup, and clinical symptoms and signs are required in every case. Adrenocortical carcinoma remains a real concern but is restricted to <2% of all cases. Functional adrenal incidentaloma lesions are commoner (but still probably <10% of total) and the greatest challenge remains the diagnosis and optimum management of autonomous cortisol secretion. Modern-day surgery has improved outcomes and novel radiological and urinary biomarkers will improve early detection and patient stratification in future years to come.
Keywords: adrenal adenoma; adrenal computed tomography; adrenal cortical carcinoma; adrenal incidentaloma; autonomous cortisol secretion.
© Endocrine Society 2020.
Figures
References
-
- Papanicolas I, Woskie LR, Jha AK. Health care spending in the united states and other high-income countries. JAMA. 2018;319(10):1024-1039. - PubMed
-
- Operational Information for Commissioning NE . Diagnostic Imaging Dataset Statistical Release: Provisional monthly statistics, November 2017 to November 2018. 2019.. https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2019/12....
-
- Fassnacht M, Arlt W, Bancos I, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2016;175(2):G1-G34. - PubMed
-
- Geelhoed GW, Druy EM. Management of the adrenal “incidentaloma”. Surgery. 1982;92(5):866-874. - PubMed
