

Assessment of Vancomycin Pharmacokinetics and Dose Regimen Optimisation in Preterm Neonates
- PMID: 32266599
- PMCID: PMC7221111
- DOI: 10.1007/s40268-020-00302-7
Assessment of Vancomycin Pharmacokinetics and Dose Regimen Optimisation in Preterm Neonates
Abstract
Background: The pharmacokinetics of vancomycin, a drug used for the treatment of methicillin-resistant Staphylococcus aureus (MRSA), varies between paediatric and adult patients.
Objective: The objective of this study was to assess the pharmacokinetics of vancomycin in preterm neonates and determine the optimum dose regimen.
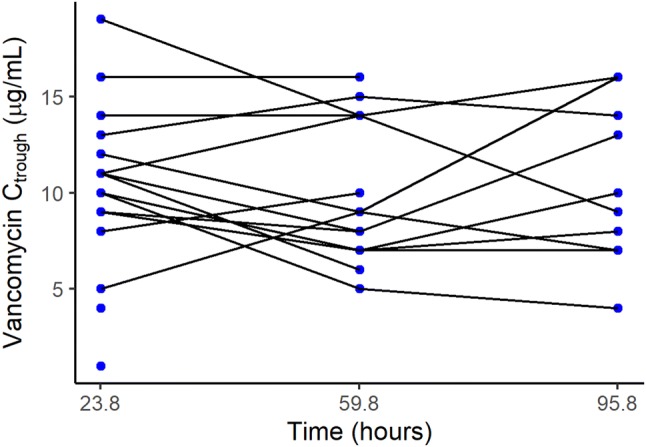
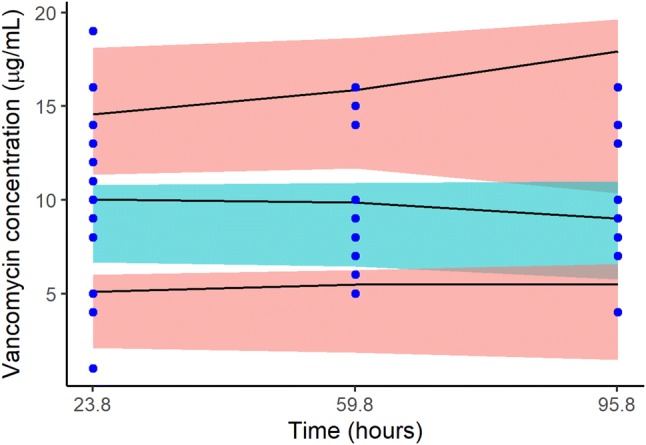
Methods: This was a randomised double-blind study of preterm neonates admitted to neonatal intensive care units. They all received vancomycin 15 mg/kg every 12 h. Blood was sampled just before administration of the third, sixth and ninth vancomycin dose. Pharmacokinetic parameters were estimated using a Bayesian approach implemented in Monolix 2018R2 software. Covariates assessed included postmenstrual age, current weight, creatinine clearance, albumin, gestational age, body surface area and current age. We used Monte Carlo simulations for dose regimen optimisation targeting area under the concentration-time curve up to 24 h (AUC0-24h) of ≥ 400 mg × h/L.
Results: In total, 19 preterm neonates were enrolled in the study with a median age of 14 (3-58) days. A one-compartment model with linear elimination best described the pharmacokinetics of vancomycin. Volume of distribution and clearance was 0.88 L and 0.1 L/h, respectively, for a typical neonate weighing 1.48 kg. Simulation of the current dose regimen showed that 27.5% of the neonates would achieve the target AUC0-24h of ≥ 400 mg × h/L, and 70.7% of the neonates would achieve it with 12 mg/kg every 8 h.
Conclusion: The majority of the neonates were under dosed. Vancomycin 12 mg/kg should be administered every 8 h over 1 h infusion to improve the likelihood of achieving the AUC0-24h target of ≥ 400 mg × h/L. This target is considered optimal for MRSA infections, where the vancomycin minimum inhibitory concentration is ≤ 1 µg/mL.
Conflict of interest statement
Mwila Mulubwa, Heletje Aletta Griesel, Pierre Mugabo, Ricky Dippenaar, and Lizelle van Wyk have no conflicts of interest that are directly relevant to the content of this article.
Figures


References
-
- Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52:e18–e55. doi: 10.1093/cid/ciq146. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
