

Occurrence of pendelluft under pressure support ventilation in patients who failed a spontaneous breathing trial: an observational study
- PMID: 32266600
- PMCID: PMC7138895
- DOI: 10.1186/s13613-020-00654-y
Occurrence of pendelluft under pressure support ventilation in patients who failed a spontaneous breathing trial: an observational study
Abstract
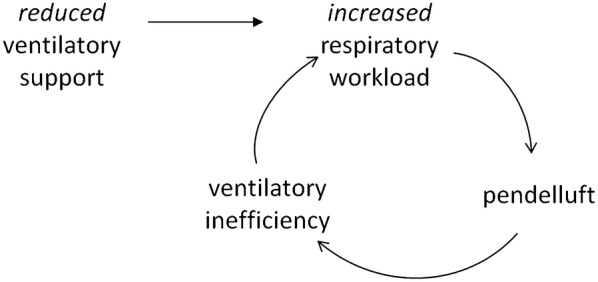
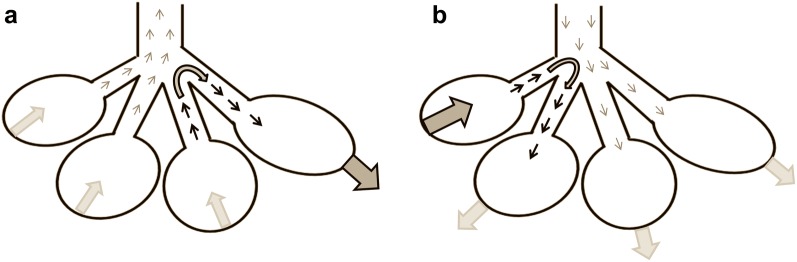
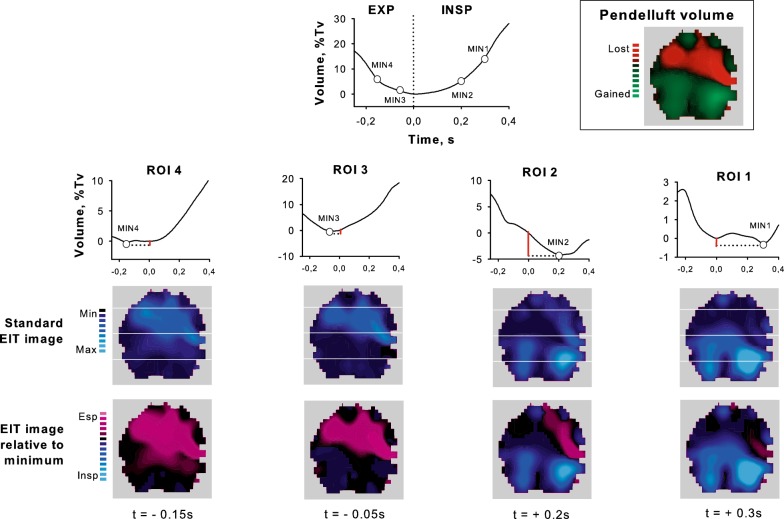
Background: Pendelluft, the movement of gas within different lung regions, is present in animal models of assisted mechanical ventilation and associated with lung overstretching. Due to rebreathing of CO2 as compared to fresh gas, pendelluft might reduce ventilatory efficiency possibly exacerbating patient's respiratory workload during weaning. Our aim was to measure pendelluft by electrical impedance tomography (EIT) in patients who failed a spontaneous breathing trial (SBT).
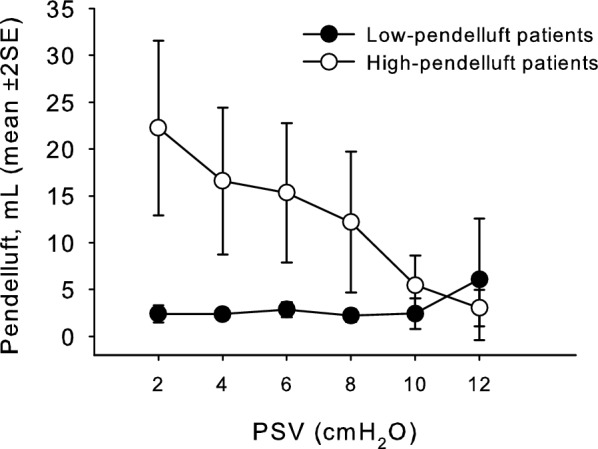
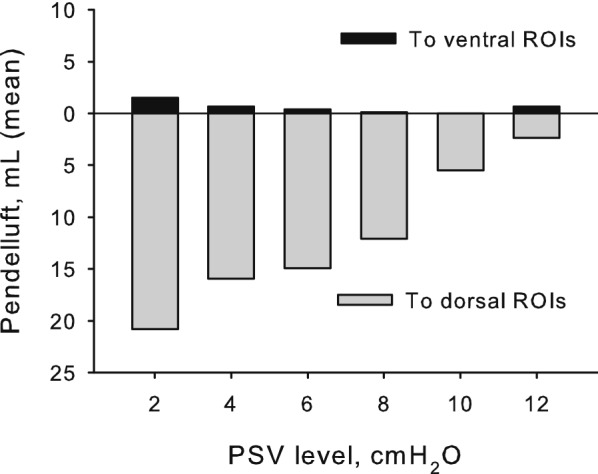
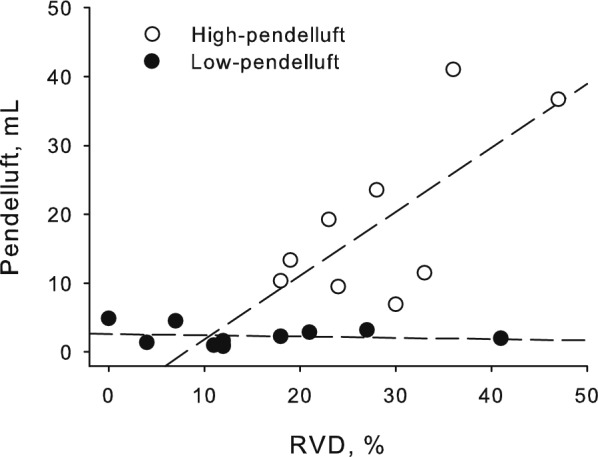
Methods: This is an observational study conducted in a general intensive care unit of a tertiary-level teaching hospital. EIT signal was recorded in 20 patients while pressure support (PS) ventilation was progressively reduced from clinical level (baseline) to 2 cmH2O, as in an SBT; four ventral-to-dorsal lung regions of interest were identified for pendelluft measurement. A regional gas movement (> 6 mL) occurring in a direction opposite to the global EIT signal was considered diagnostic for high pendelluft.
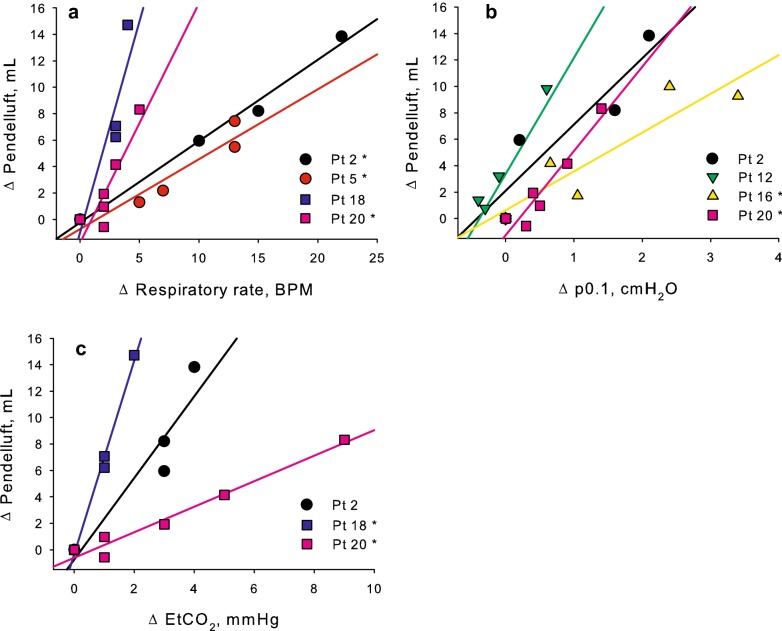
Results: Eight patients out of 20 (40%) were classified as high-pendelluft; baseline clinical characteristics did not differ between high- and low-pendelluft patients. At PS reduction, pendelluft and EtCO2 increased more in the high-pendelluft group (p < .001 and .011, respectively). The volume of gas subject to pendelluft moved almost completely from the ventral towards the dorsal lung regions, while the opposite movement was minimal (16.3 [10:32.8] vs. 0 [0:1.8] mL, p = .001). In a subgroup of patients, increased pendelluft volumes positively correlated with markers of respiratory distress such as increased respiratory rate, p0.1, and EtCO2.
Conclusions: Occult pendelluft can be measured by EIT, and is frequently present in patients failing an SBT. When present, pendelluft increases with the reduction of ventilator support and is associated with increased EtCO2, suggesting a reduction of the ability to eliminate CO2.
Keywords: Assisted mechanical ventilation; Difficult ventilator weaning; Electrical impedance tomography; Pendelluft; Spontaneous assisted breathing; Spontaneous breathing trial.
Conflict of interest statement
GB, AB and GF received lecturing fees from Draeger Medical.
Figures
References
-
- Lumb A. Nunn’s Applied Respiratory Physiology. Amsterdam: Elsevier; 2016. Causes of time dependence of pulmonary elastic behaviour; p. 24.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
