Patient-Reported Outcomes in an Observational Cohort of HIV-1-Infected Adults on Darunavir/Cobicistat-Based Regimens: Beyond Viral Suppression
- PMID: 32266663
- PMCID: PMC7210246
- DOI: 10.1007/s40271-020-00413-y
Patient-Reported Outcomes in an Observational Cohort of HIV-1-Infected Adults on Darunavir/Cobicistat-Based Regimens: Beyond Viral Suppression
Erratum in
-
Correction to: Patient-Reported Outcomes in an Observational Cohort of HIV-1-Infected Adults on Darunavir/Cobicistat-Based Regimens: Beyond Viral Suppression.Patient. 2020 Aug;13(4):469-470. doi: 10.1007/s40271-020-00425-8. Patient. 2020. PMID: 32468416 Free PMC article.
Abstract
Objective: This prospective, multicenter, non-interventional cohort study enrolling human immunodeficiency virus (HIV)-1-infected, virally suppressed adult outpatients in Italy aimed to describe results obtained from patient-reported outcome questionnaires regarding treatment satisfaction and symptom perceptions in HIV-1-positive patients who switched to cobicistat-boosted darunavir antiretroviral regimens, coming from ritonavir-boosted protease inhibitors.
Methods: Patients entered this study between June 2016 and February 2017, once their treating physician had considered them eligible for cobicistat-boosted darunavir-based treatment as per clinical practice. Patients' satisfaction regarding regimen and current symptom burdens were assessed using two previously validated, patient-reported outcome questionnaires: HIV Treatment Satisfaction Questionnaire (HIV-TSQ) and HIV Symptoms Distress Module (HIV-SDM). These questionnaires were administered at prespecified time-points: enrollment (Visit 1), 4-8 weeks later (Visit 2), and 48 ± 6 weeks after study enrollment (Visit 4). Data of patient-reported outcome total scores for both questionnaires are presented as median with 25th-75th percentiles. Questionnaires scores were analyzed overall and stratified by gender when applicable. A p value of less than 0.05 was considered statistically significant. A sensitivity analysis was conducted to evaluate the role of lost to follow-up, using the "last observation carried forward" method.
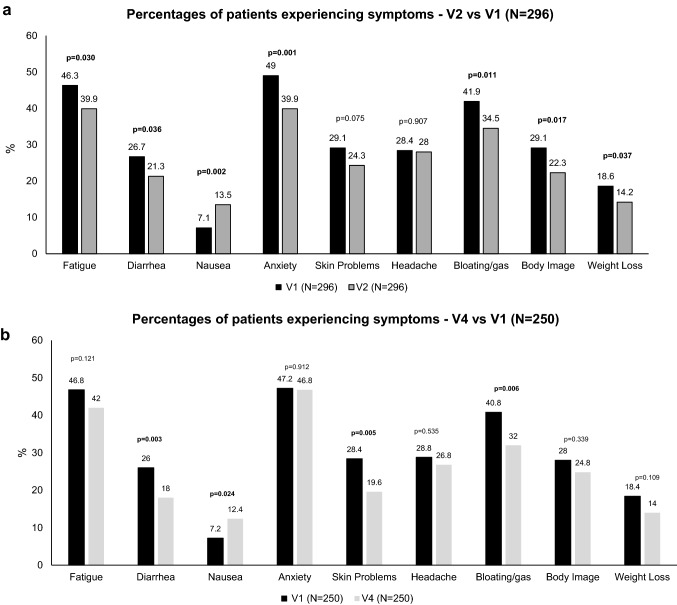
Results: A total of 348 patients were enrolled in this study; 296 patients (208 male and 88 female) provided both evaluable HIV-TSQ and HIV-SDM at enrollment and at 4-8 weeks, while 250 patients (174 male and 76 female) provided questionnaire data at enrollment and at 48 ± 6 weeks. The total scores of HIV-TSQ showed improvements in patient satisfaction in the overall population both at Visit 2 and Visit 4 (p < 0.001, sign test) and also when stratified by gender throughout the study period. In addition, the overall burden of symptoms, as shown by the HIV-SDM scores, decreased.
Conclusions: Switching to a cobicistat-boosted darunavir-based therapy led to overall increased patient satisfaction and reduced symptom burden when compared with previous regimens. The use of patient-reported outcomes in clinical daily practice could provide a useful tool towards achieving guideline goals to achieve "fourth 90", having 90% of virally suppressed patients with a good health-related quality of life.
Conflict of interest statement
Andrea Antinori received a grant from Gilead Sciences, ViiV Healthcare, and Janssen-Cilag; he received consulting fees or honorarium from ViiV Healthcare, Janssen-Cilag, and Merck. Emanuele Foca has received consultancy fees and honoraria by several pharmaceutical companies in the field of HIV infections. Annamaria Cattelan received a grant from Janssen-Cilag and consulting fees or honorarium from ViiV Healthcare, MSD, Gilead Sciences, and Janssen-Cilag. Giordano Madeddu received consulting fees or honorarium from ViiV Healthcare, Gilead Sciences, MSD, and Janssen-Cilag; he received a speaker’s fee from ViiV Healthcare, Angelini, and Pfizer. Emanuele Pontali received consulting fees or honorarium for advisory board participation for Janssen-Cilag; he received payments for training activities for Janssen-Cilag. Barbara Rossetti received consulting fees or honorarium for educational activities with REPs and a support for meeting participation. Andrea Gori received a grant from Janssen-Cilag, ViiV Healthcare, MSD, BMS, Abbvie, Gilead Sciences, Novartis, Pfizer, Astellas, AstraZeneca, and Angelini; he received consulting fees or honorarium from Janssen-Cilag, ViiV Healthcare, MSD, BMS, Abbvie, Gilead Sciences, Novartis, Pfizer, Astellas, AstraZeneca, and Angelini. Maria V. Cossu, Barbara Menzaghi, Gaetana Sterrantino, Nicola Squillace, Valentina Di Cristo, Antonella Catagna, Giancarlo Orofino, Daniela Valenti, Gabriella D’Ettore, Lucia Aprea, Sergio Ferrara, Maria E. Locatelli, Paolo Scerbo, and Francesco Rucci have no conflicts of interest that are directly relevant to the content of this article. Alessia Uglietti, Roberta Termini, and Daniela Mancusi are Janssen employees.
Figures