

Efficacy, safety and cardiovascular outcomes of once-daily oral semaglutide in patients with type 2 diabetes: The PIONEER programme
- PMID: 32267058
- PMCID: PMC7384149
- DOI: 10.1111/dom.14054
Efficacy, safety and cardiovascular outcomes of once-daily oral semaglutide in patients with type 2 diabetes: The PIONEER programme
Abstract
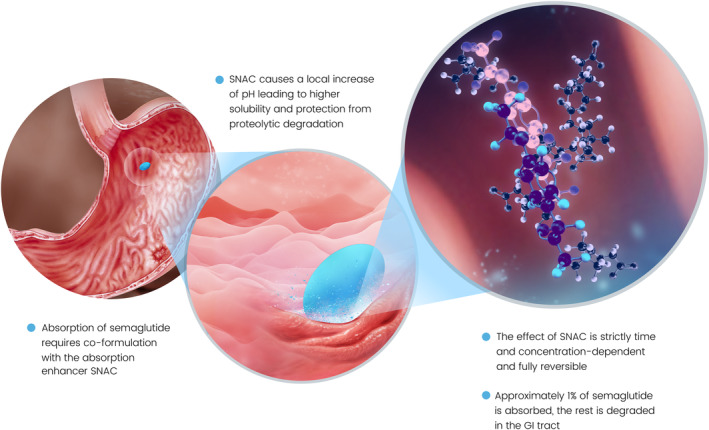
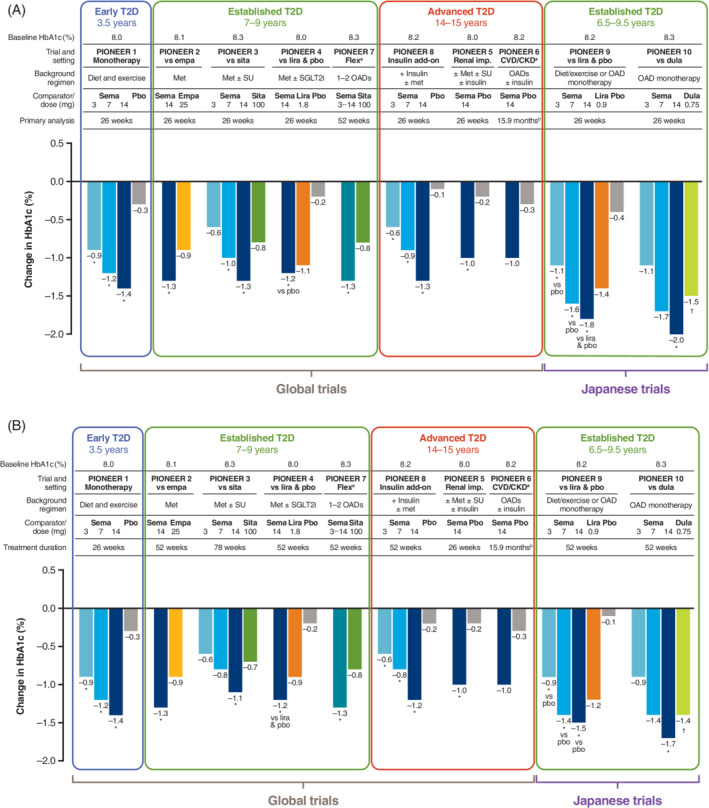
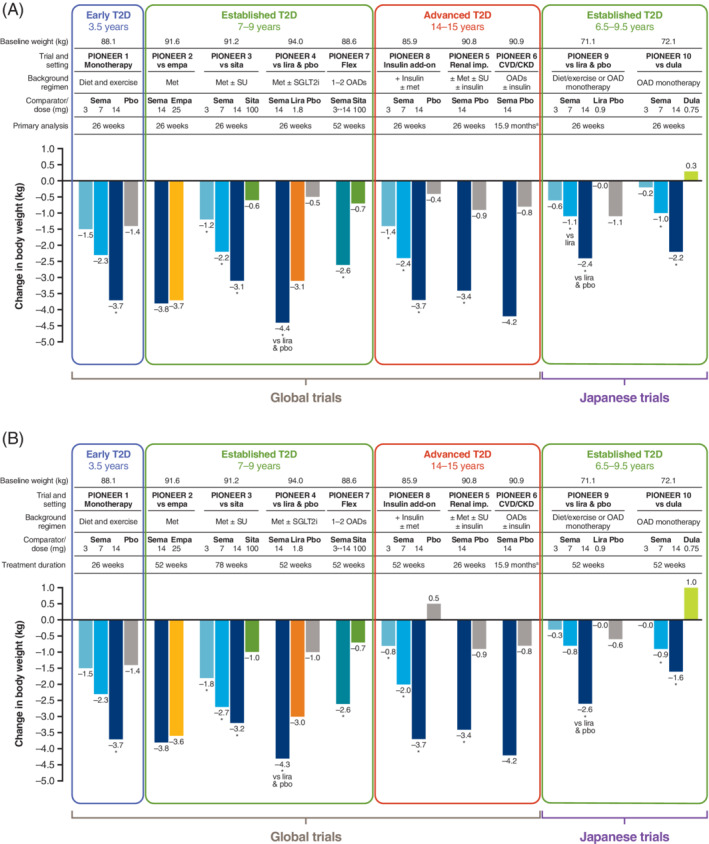
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are recommended for glycaemic management in patients with type 2 diabetes (T2D). Oral semaglutide, the first oral GLP-1RA, has recently been approved for clinical use, based on the results of the randomized, Phase 3a Peptide InnOvatioN for Early diabEtes tReatment (PIONEER) clinical trials. The PIONEER programme tested oral semaglutide in patients with T2D of duration ranging from 3.5 to 15 years, from monotherapy through to insulin add-on, in global populations and two trials dedicated to Japanese patients. Outcomes (glycated haemoglobin [HbA1c] and body weight reduction, plus other relevant efficacy and safety endpoints) were tested against both placebo and active standard-of-care medications. A separate trial evaluated the cardiovascular safety of oral semaglutide in patients with T2D at high cardiovascular risk. Over periods of treatment up to 78 weeks, oral semaglutide 7 and 14 mg once daily reduced HbA1c and body weight across the spectrum of T2D, and improved other diabetes-related endpoints, such as fasting plasma glucose. Oral semaglutide provided significantly better efficacy than placebo and commonly used glucose-lowering medications from the dipeptidyl peptidase-4 inhibitor (sitagliptin) and sodium-glucose co-transporter-2 inhibitor (empagliflozin) classes, as well as the subcutaneous GLP-1RAs liraglutide and dulaglutide. Oral semaglutide was well tolerated in line with the known safety profile of GLP-1RAs, with transient gastrointestinal events being the most common side effects reported. Cardiovascular safety was demonstrated for oral semaglutide in patients with cardiovascular disease or high cardiovascular risk. The results of the PIONEER programme suggest that oral semaglutide is efficacious and well tolerated for glycaemic control of T2D. The availability of oral semaglutide may help to broaden treatment choice and facilitate adoption of earlier GLP-1RA treatment in the paradigm of T2D management.
Trial registration: ClinicalTrials.gov NCT02906930 NCT02863328 NCT02607865 NCT02863419 NCT02827708 NCT02692716 NCT02849080 NCT03021187 NCT03018028 NCT03015220.
Keywords: GLP-1 analogue; Phase 3 study; cardiovascular disease; clinical trial; type 2 diabetes.
© 2020 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
T.K.T. is on the speaker's bureau for Novo Nordisk and is one of the US national leads for the Semaglutide Cardiovascular Outcomes Trial in Patients With Type 2 Diabetes (SOUL) trial (NCT03914326). R.P. has received lecture and consulting fees from AstraZeneca; consulting fees from Boehringer Ingelheim, Eisai, GlaxoSmithKline and Mundipharma; grants and lecture/consulting fees from Glytec, Janssen, Novo Nordisk, Pfizer and Takeda; grants from Lexicon Pharmaceuticals; and grants and consulting fees from Ligand Pharmaceuticals, Lilly, Merck and Sanofi‐Aventis US. Except for consulting fees in February 2018 and June 2018 received from Sanofi US Services, all fees for services were paid directly to AdventHealth, a non‐profit organization. J.J.M. has received lecture honoraria and consulting fees from AstraZeneca, Berlin‐Chemie, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme (MSD), Novo Nordisk, Novartis and Sanofi; has received reimbursement of congress participation fees and travel expenses from MSD, Novo Nordisk and Sanofi; and has initiated projects supported by Boehringer Ingelheim, MSD, Novo Nordisk and Sanofi.
Figures
References
-
- Drucker DJ, Nauck MA. The incretin system: glucagon‐like peptide‐1 receptor agonists and dipeptidyl peptidase‐4 inhibitors in type 2 diabetes. Lancet. 2006;368(9548):1696‐1705. - PubMed
-
- Buse JB, Wexler DJ, Tsapas A, et al. 2019 update to: management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2020;63(2):221‐228. - PubMed
-
- American Diabetes Association . 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes‐2020. Diabetes Care. 2020;43(Suppl 1):S98‐S110. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
