Association Between Lifetime Affective Symptoms and Premature Mortality
- PMID: 32267482
- PMCID: PMC7142795
- DOI: 10.1001/jamapsychiatry.2020.0316
Association Between Lifetime Affective Symptoms and Premature Mortality
Abstract
Importance: Associations between affective symptoms and mortality have been evaluated, but studies have not examined timing or cumulative exposure to affective symptoms over the life course.
Objectives: To examine how lifetime accumulation and timing of affective symptoms are associated with mortality and identify potential explanatory factors.
Design, setting, and participants: Data were obtained from the MRC National Survey of Health and Development (1946 British birth cohort), a socially stratified, population-based sample originally consisting of 5362 singleton births in England, Wales, and Scotland during March 1946. The cohort has been followed up 24 times, most recently in 2014-2015. Eligible participants included those flagged for mortality with affective symptom data available at a minimum of 3 time points (n = 3001). Data analysis was conducted from July 2016 to January 2019.
Exposures: Affective symptoms were assessed at ages 13 to 15 years (teacher-rated questionnaire), 36 years (Present State Examination clinical semistructured interview), 43 years (Psychiatric Symptom Frequency questionnaire), and 53 years (General Health Questionnaire-28). Case-level affective symptoms were determined by those scoring in the top 16th percentile (ie, suggestive of a clinical diagnosis).
Main outcomes and measures: Mortality data were obtained from the UK National Health Service Central Register from age 53 to 68 years.
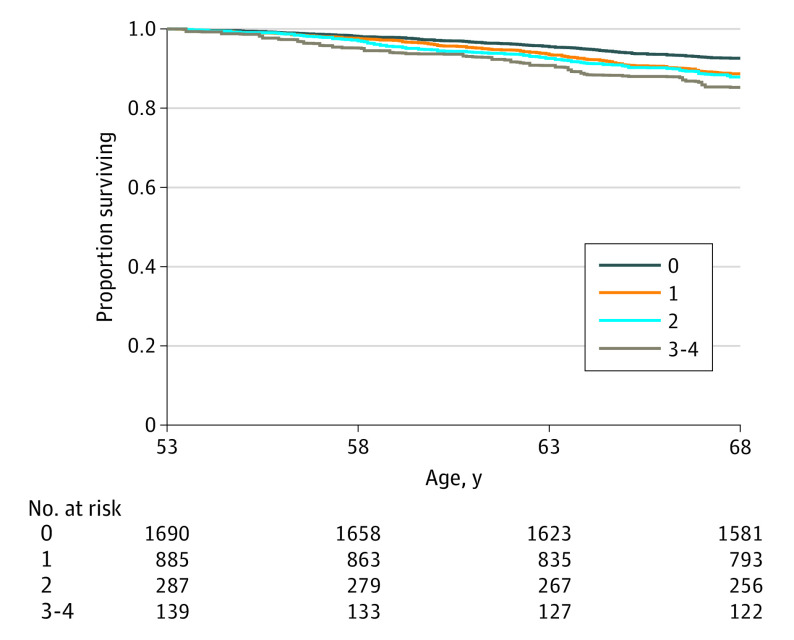
Results: Of 3001 study members (1509 [50.3%] female, 1492 [49.7%] male), 235 individuals (7.8%) died over a 15-year follow-up. After adjustment for sex, those who experienced case-level affective symptoms 1, 2, and 3 to 4 times had 76%, 87%, and 134% higher rates of premature mortality, respectively, compared with those who never experienced case-level symptoms. Case-level symptoms in adolescence only (ages 13-15 years) were associated with a 94% increased rate of mortality, which was unexplained after full adjustment for covariates (hazard ratio, 1.73; 95% CI, 1.10-2.72). Associations between participants with case-level symptoms multiple (2-4) times and mortality were predominately explained by adult health indicators and behaviors. For example, associations for those with case-level symptoms 3 to 4 times were most strongly attenuated by number of health conditions (32.1%), anxiolytic use (28.4%), lung function (24.6%), physical activity (23.9%), smoking (24.6%), antidepressant use (20.1%), diet (16.4%), pulse rate (12.7%), and adult social class (11.2%).
Conclusions and relevance: Lifetime accumulation of affective symptoms may be associated with an increased rate of mortality, with explanatory pathways dependent on the duration and timing of symptoms. Future research into causal pathways and potential points of intervention should consider affective symptom history.
Conflict of interest statement
Figures