

Cytologic grading of primary malignant salivary gland tumors: A blinded review by an international panel
- PMID: 32267606
- PMCID: PMC7413070
- DOI: 10.1002/cncy.22271
Cytologic grading of primary malignant salivary gland tumors: A blinded review by an international panel
Abstract
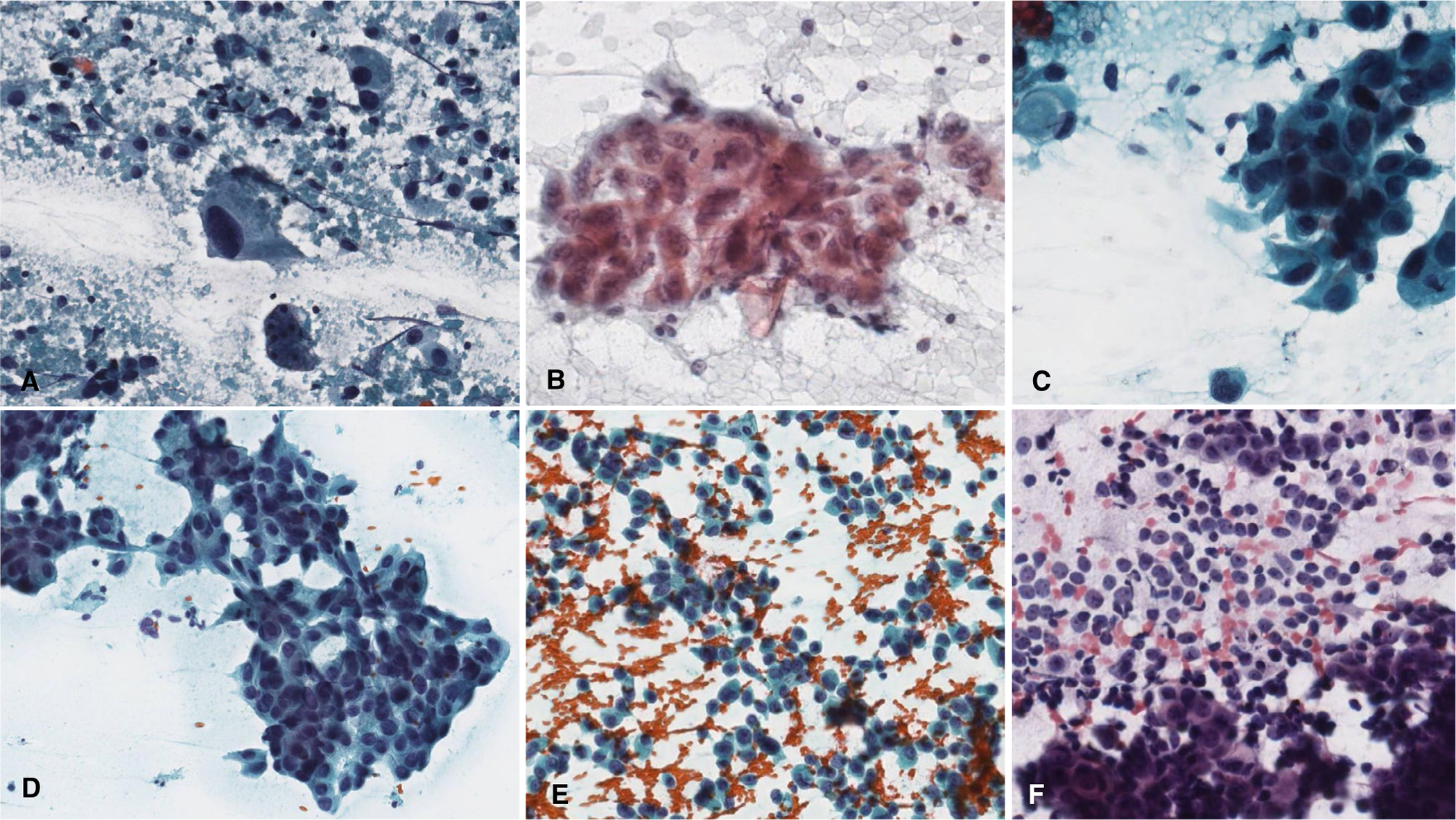
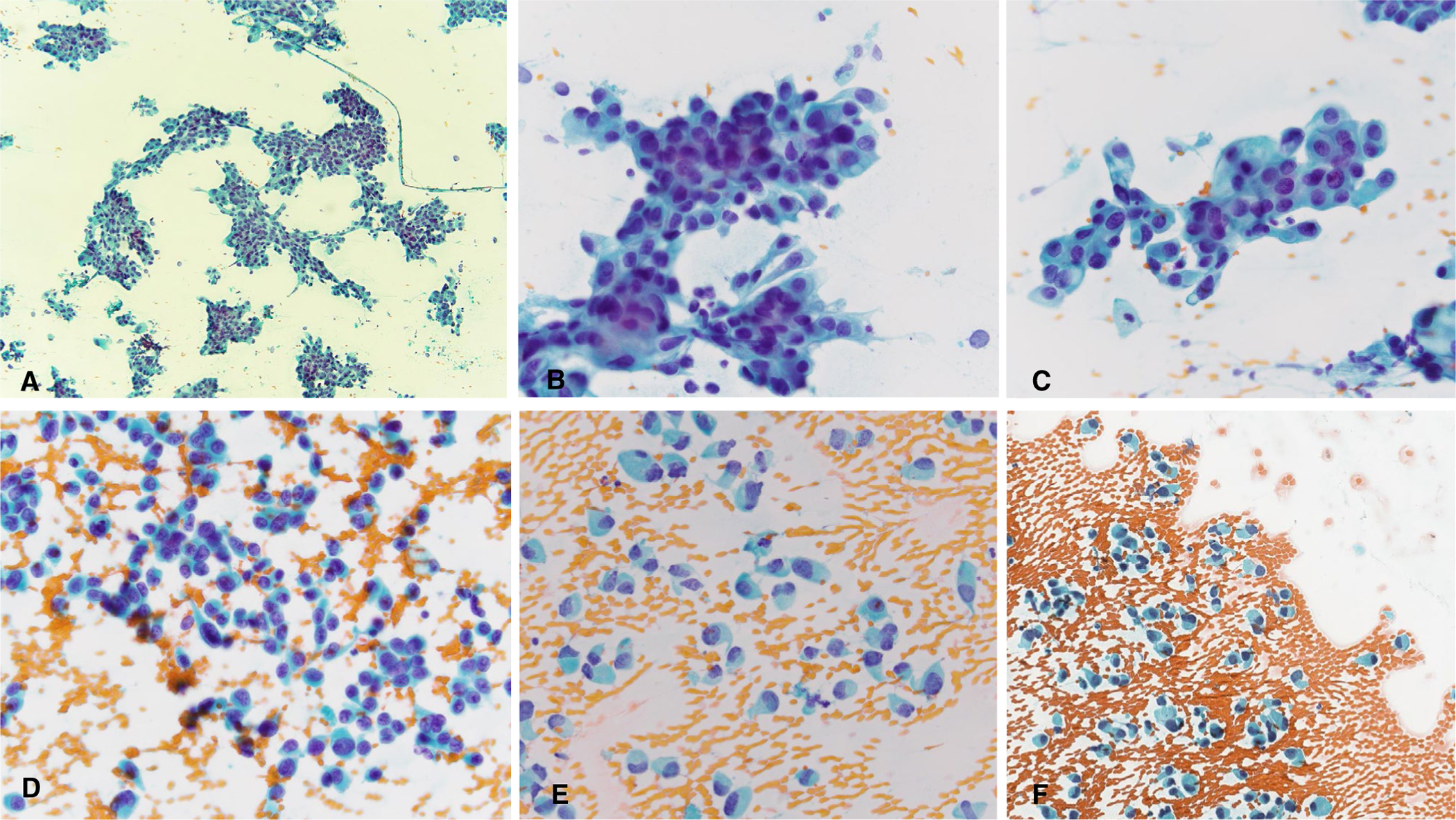
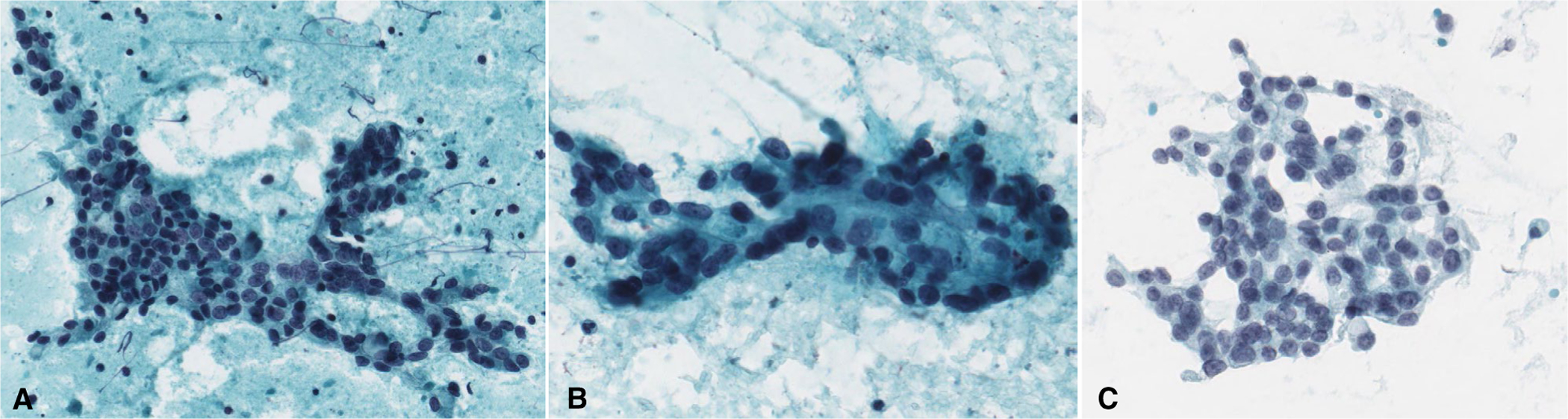
Background: Fine needle aspiration (FNA) is commonly used for the preoperative evaluation of salivary gland tumors. Tumor grade is a key factor influencing clinical management of salivary gland carcinomas (SGCs). To assess the ability to grade nonbasaloid SGCs in FNA specimens, an international panel of cytopathologists convened to review and score SGC cases.
Methods: The study cohort included 61 cases of primary SGC from the pathology archives of 3 tertiary medical centers. Cases from 2005 to 2016 were selected, scanned, and digitized. Nineteen cytopathologists blinded to the histologic diagnosis reviewed the digitized cytology slides and graded them as low, high, or indeterminate. The panelists' results were then compared to the tumor grades based on histopathologic examination of the corresponding resection specimens.
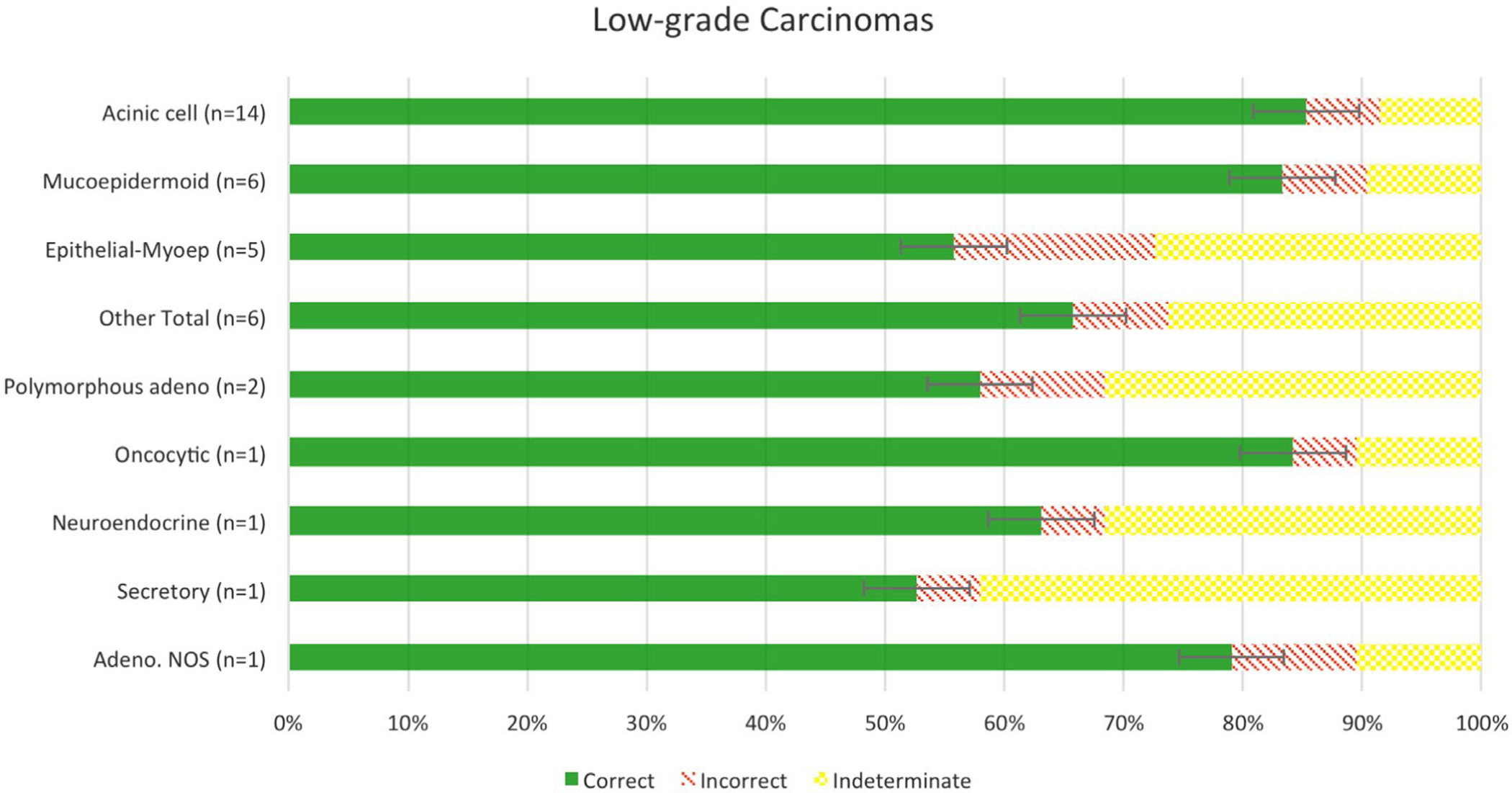
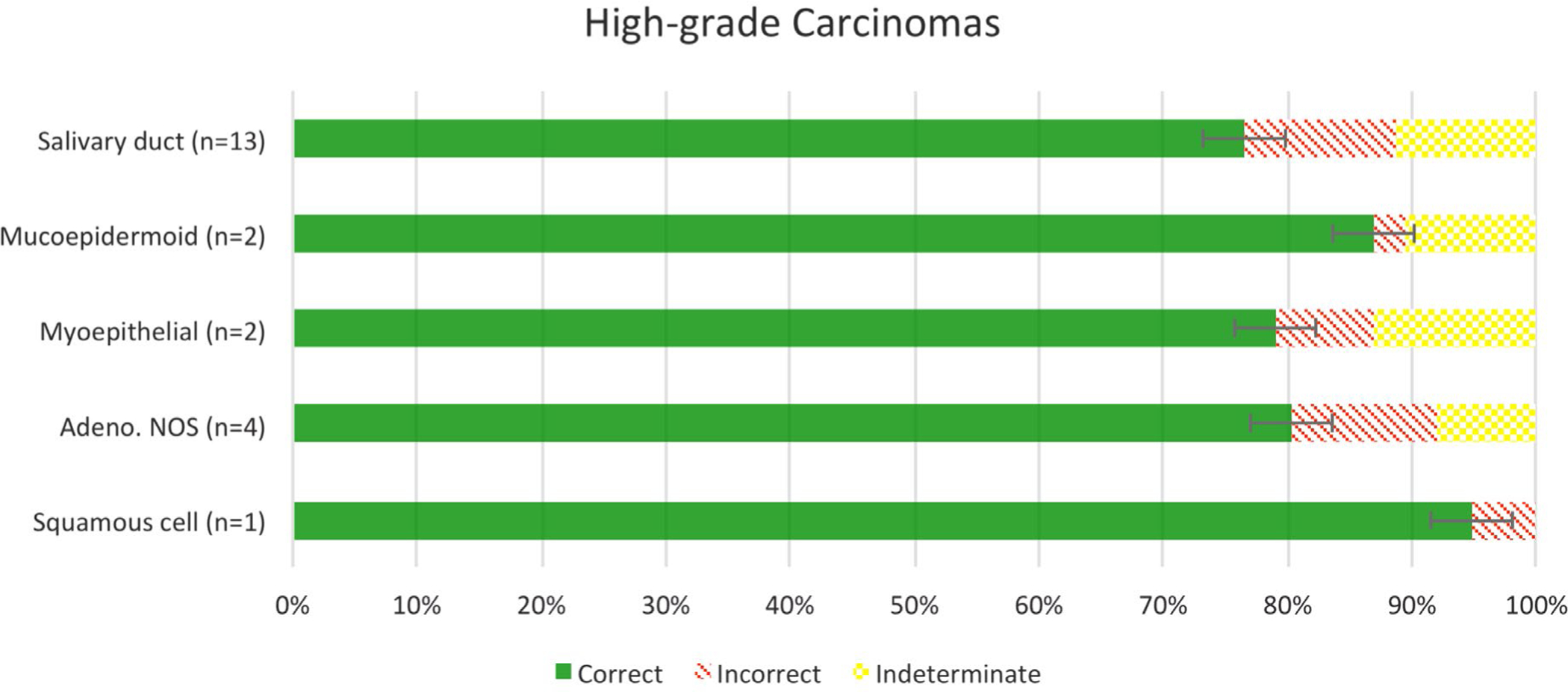
Results: All but 2 of the 19 (89.5%) expert panelists review more than 20 salivary gland FNAs per year; 16 (84.2%) of the panelists work at academic medical centers, and 13 (68.4%) have more than 10 years' experience. Participants had an overall accuracy of 89.4% in the grading of SGC cases, with 90.2% and 88.3% for low- and high-grade SGC, respectively. Acinic cell carcinoma and mucoepidermoid carcinoma had the highest degree of accuracy, while epithelial-myoepithelial carcinoma and salivary duct carcinoma had the lowest degree of accuracy. As expected, the intermediate-grade SGC cases showed the greatest variability (high-grade, 42.1%; low-grade, 37.5%, indeterminate, 20.4%).
Conclusion: This study confirms the high accuracy of cytomorphologic grading of primary SGC by FNA as low- or high-grade. However, caution should be exercised when a grade cannot be confidently assigned.
Keywords: FNA; Milan system; cancer; cytology; grading; salivary gland.
© 2020 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
The authors made no disclosures.
Figures
References
-
- Tyagi R, Dey P. Diagnostic problems of salivary gland tumors. Diagn Cytopathol. 2015;43:495–509. - PubMed
-
- Seethala RR. Basaloid/blue salivary gland tumors. Mod Pathol. 2017;30(suppl 1):S84–S95. - PubMed
-
- Skálová A, Gnepp DR, Lewis JS, et al. Newly described entities in salivary gland pathology. Am J Surg Pathol. 2017;41:e33–e47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
