

Influence of sickle cell disease on susceptibility to HIV infection
- PMID: 32267841
- PMCID: PMC7141606
- DOI: 10.1371/journal.pone.0218880
Influence of sickle cell disease on susceptibility to HIV infection
Abstract
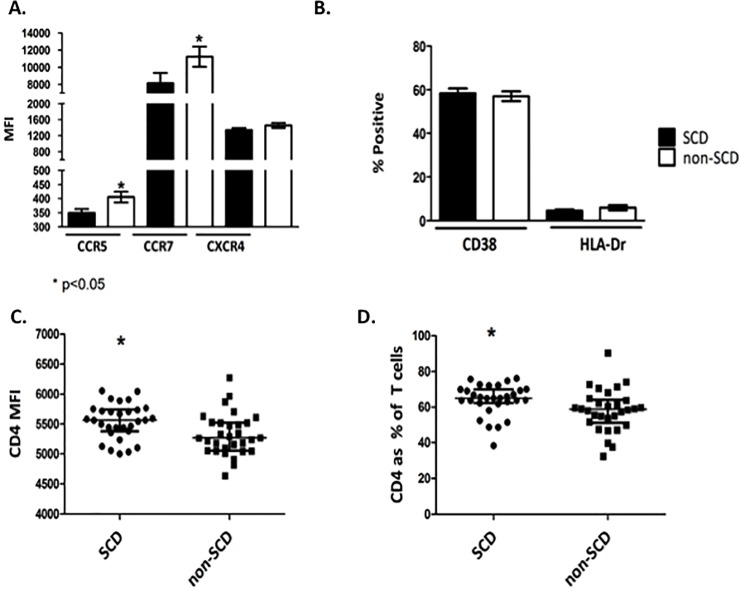
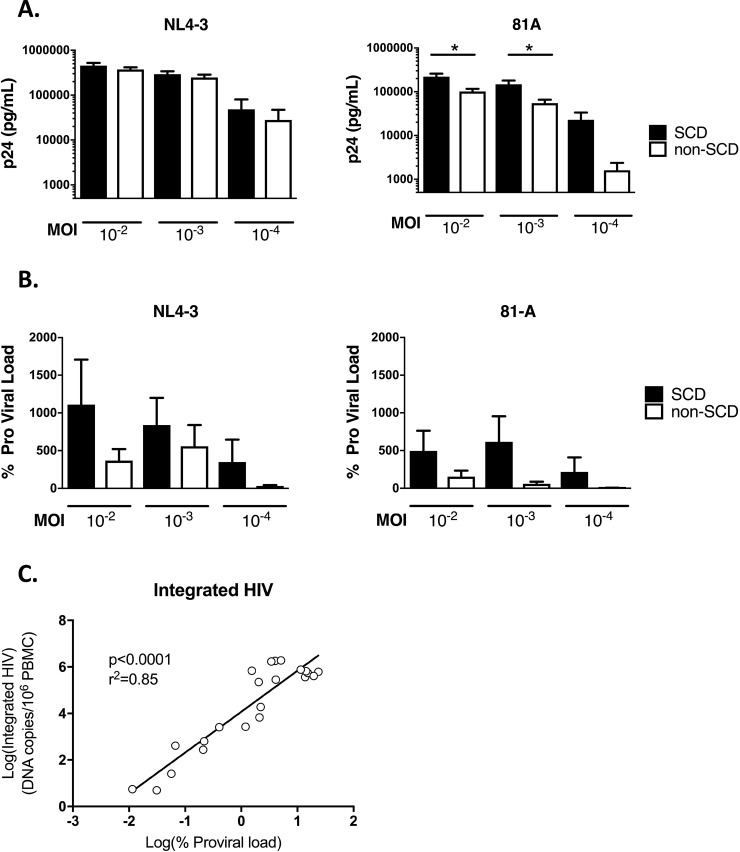
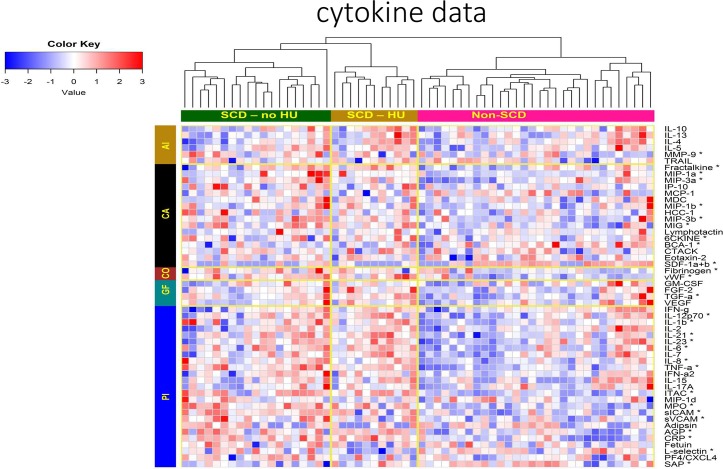
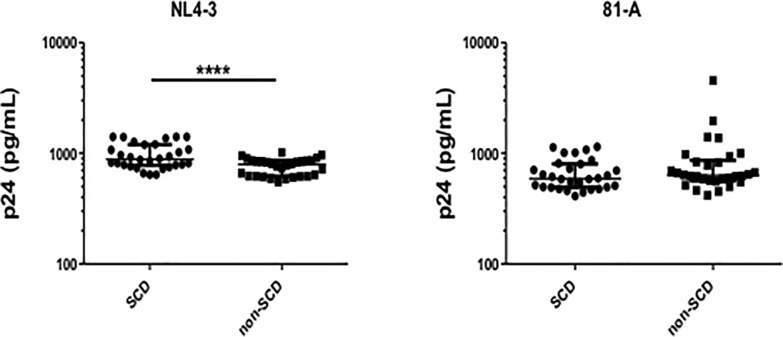
People with sickle cell disease (SCD) are reported to have low rates of HIV infection, slower progression to AIDS and lower HIV-associated mortality compared to the general population. Mechanisms of potential resistance to HIV in SCD are incompletely understood. We retrospectively reviewed the Transfusion Safety Study to compare HIV status between people with SCD and other congenital anemias who were routinely exposed to blood products during the high-risk period before HIV screening implementation. Non-SCD congenital anemia diagnosis was associated with a higher risk of HIV acquisition compared to SCD (OR 13.1 95%CI 1.6-108.9). In addition, we prospectively enrolled 30 SCD cases and 30 non-SCD controls to investigate potential mechanisms of resistance to HIV in SCD. CCR5 and CCR7 expression was lower and CD4 expression was higher on CD4+ T cells from SCD cases compared to controls. Surface expression of CD4+ T cell CXCR4, CD38 and HLA-DR did not differ between the groups. SCD CD4+ T cells were not less susceptible to HIV infection than controls. Levels of multiple cytokines were elevated in the SCD plasma, but SCD plasma compared to control plasma did not inhibit HIV infection of target cells. In conclusion, our epidemiological data support people with SCD being resistant to HIV infection. Potential mechanisms include lower CD4+ T cell expression of CCR5 and CCR7, balanced by increased CD4 expression and cytokine levels, which did not result in in vitro resistance to HIV infection. Further study is needed to define the risk and pathophysiology of HIV in persons with SCD.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Waweru SEN KD, Kitoyi GW. Absence of HIV seropositivity in children with sickle cell anemia at Kenyatta National Hospital. Internation AIDS Conference. 1989:248.
-
- Waweru SEN ME, Libondo J. Persistent low HIV infection in transfused sicklers as compared to high HIV infection in children presenting with other types of aneamia requiring blood transfusion. Nairob J Med. 1992;8:26.
-
- Batina Agasa S, Dupont E, Kayembe T, Molima P, Malengela R, Kabemba S, et al. Multiple transfusions for sickle cell disease in the Democratic Republic of Congo: the importance of the hepatitis C virus. Transfusion clinique et biologique: journal de la Societe francaise de transfusion sanguine. 2010;17(4):254–9. 10.1016/j.tracli.2010.09.002 . - DOI - PubMed
-
- Castro O, Saxinger C, Barnes S, Alexander S, Flagg R, Frederick W. Prevalence of antibodies to human immunodeficiency virus and to human T cell leukemia virus type I in transfused sickle cell disease patients. The Journal of infectious diseases. 1990;162(3):743–5. 10.1093/infdis/162.3.743 . - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
