

Prevalence and outcome of dual aortic stenosis and cardiac amyloid pathology in patients referred for transcatheter aortic valve implantation
- PMID: 32267922
- PMCID: PMC7395329
- DOI: 10.1093/eurheartj/ehaa170
Prevalence and outcome of dual aortic stenosis and cardiac amyloid pathology in patients referred for transcatheter aortic valve implantation
Abstract
Aims: Cardiac amyloidosis is common in elderly patients with aortic stenosis (AS) referred for transcatheter aortic valve implantation (TAVI). We hypothesized that patients with dual aortic stenosis and cardiac amyloid pathology (AS-amyloid) would have different baseline characteristics, periprocedural and mortality outcomes.
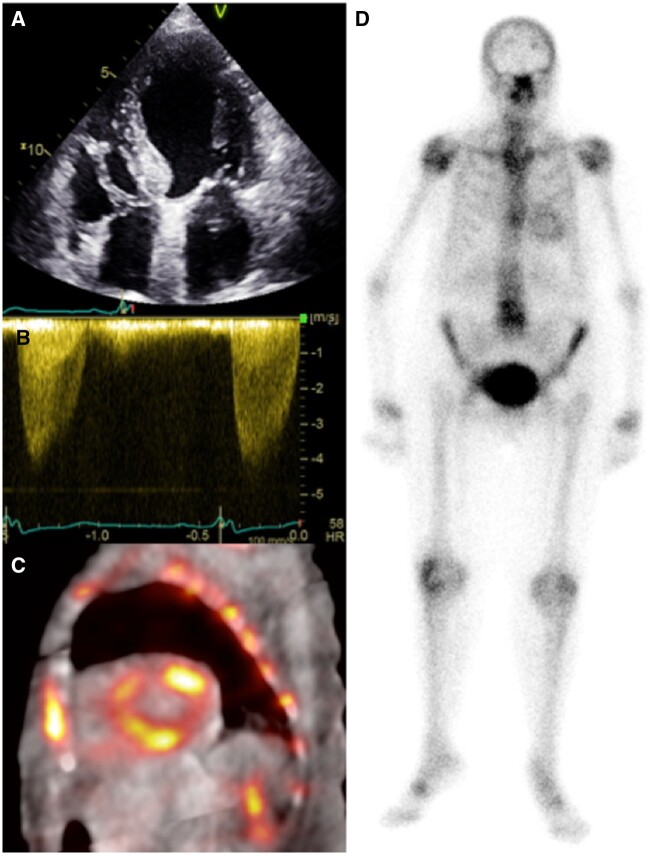
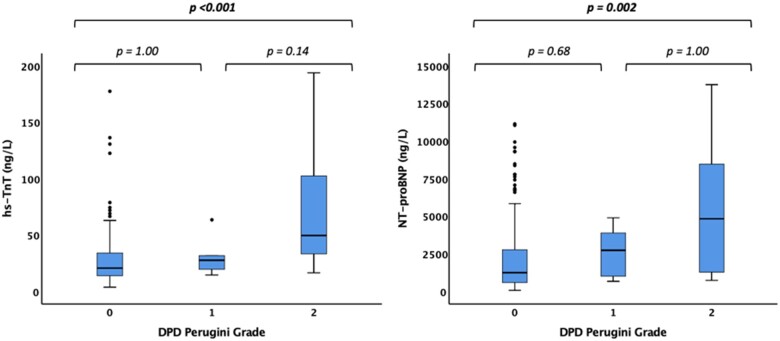
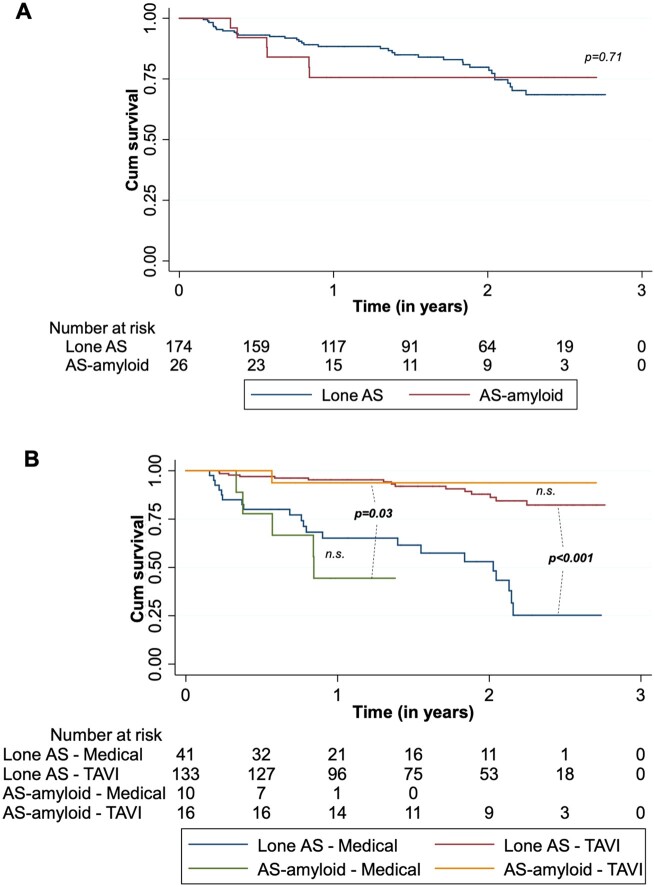
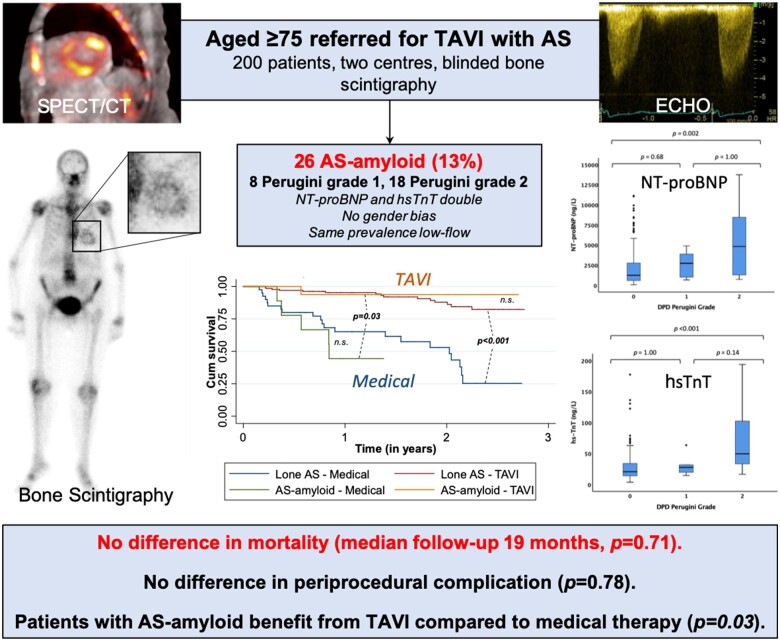
Methods and results: Patients aged ≥75 with severe AS referred for TAVI at two sites underwent blinded bone scintigraphy prior to intervention (Perugini Grade 0 negative, 1-3 increasingly positive). Baseline assessment included echocardiography, electrocardiogram (ECG), blood tests, 6-min walk test, and health questionnaire, with periprocedural complications and mortality follow-up. Two hundred patients were recruited (aged 85 ± 5 years, 50% male). AS-amyloid was found in 26 (13%): 8 Grade 1, 18 Grade 2. AS-amyloid patients were older (88 ± 5 vs. 85 ± 5 years, P = 0.001), with reduced quality of life (EQ-5D-5L 50 vs. 65, P = 0.04). Left ventricular wall thickness was higher (14 mm vs. 13 mm, P = 0.02), ECG voltages lower (Sokolow-Lyon 1.9 ± 0.7 vs. 2.5 ± 0.9 mV, P = 0.03) with lower voltage/mass ratio (0.017 vs. 0.025 mV/g/m2, P = 0.03). High-sensitivity troponin T and N-terminal pro-brain natriuretic peptide were higher (41 vs. 21 ng/L, P < 0.001; 3702 vs. 1254 ng/L, P = 0.001). Gender, comorbidities, 6-min walk distance, AS severity, prevalence of disproportionate hypertrophy, and post-TAVI complication rates (38% vs. 35%, P = 0.82) were the same. At a median follow-up of 19 (10-27) months, there was no mortality difference (P = 0.71). Transcatheter aortic valve implantation significantly improved outcome in the overall population (P < 0.001) and in those with AS-amyloid (P = 0.03).
Conclusions: AS-amyloid is common and differs from lone AS. Transcatheter aortic valve implantation significantly improved outcome in AS-amyloid, while periprocedural complications and mortality were similar to lone AS, suggesting that TAVI should not be denied to patients with AS-amyloid.
Keywords: Aortic stenosis; Cardiac amyloidosis; TAVI.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Transthyretin cardiac amyloidosis in patients with severe aortic stenosis.Eur Heart J. 2020 Aug 1;41(29):2768-2770. doi: 10.1093/eurheartj/ehaa458. Eur Heart J. 2020. PMID: 32638011 No abstract available.
-
Aortic stenosis and amyloid heart disease: 'the 2A dangerous liaisons'.Eur Heart J. 2020 Aug 1;41(29):2815. doi: 10.1093/eurheartj/ehaa549. Eur Heart J. 2020. PMID: 32738048 No abstract available.
References
-
- Lindroos M, Kupari M, Heikkilä J, Tilvis R. Prevalence of aortic valve abnormalities in the elderly: an echocardiographic study of a random population sample. J Am Coll Cardiol 1993;21:1220–1225. - PubMed
-
- Thaden JJ, Nkomo VT, Enriquez-Sarano M. The global burden of aortic stenosis. Prog Cardiovasc Dis 2014;56:565–571. - PubMed
-
- Ross J, Braunwald E. Aortic stenosis. Circulation 1968;38:61–67. - PubMed
-
- Schwarz F, Baumann P, Manthey J, Hoffmann M, Schuler G, Mehmel HC, Schmitz W, Kübler W. The effect of aortic valve replacement on survival. Circulation 1982;66:1105–1110. - PubMed
-
- Turina J, Hess O, Sepulcri F, Krayenbuehl HP. Spontaneous course of aortic valve disease. Eur Heart J 1987;8:471–483. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
