

Role of neoadjuvant chemotherapy in metastatic medulloblastoma: a comparative study in 92 children
- PMID: 32267940
- PMCID: PMC7846143
- DOI: 10.1093/neuonc/noaa083
Role of neoadjuvant chemotherapy in metastatic medulloblastoma: a comparative study in 92 children
Abstract
Background: Previous pilot studies have shown the feasibility of preoperative chemotherapy in patients with medulloblastoma, but benefits and risks compared with initial surgery have not been assessed.
Methods: Two therapeutic strategies were retrospectively compared in 92 patients with metastatic medulloblastoma treated at Gustave Roussy between 2002 and 2015: surgery at diagnosis (n = 54, group A) and surgery delayed after carboplatin and etoposide-based neoadjuvant therapy (n = 38, group B). Treatment strategies were similar in both groups.
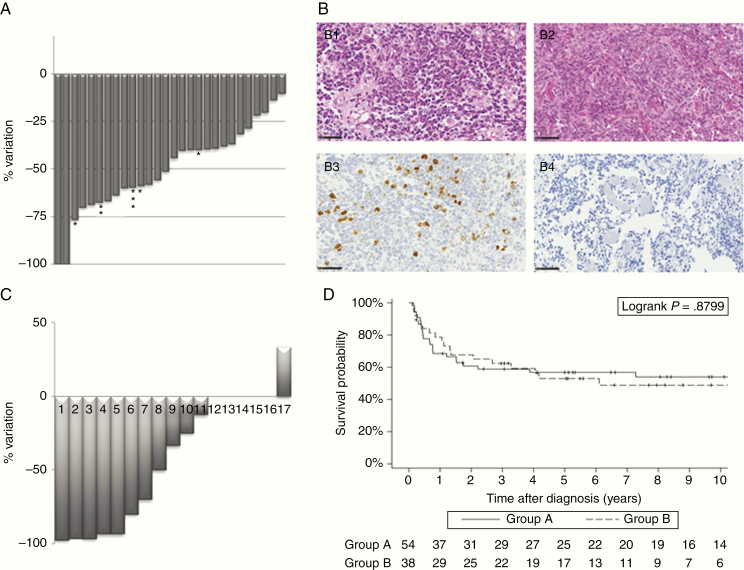
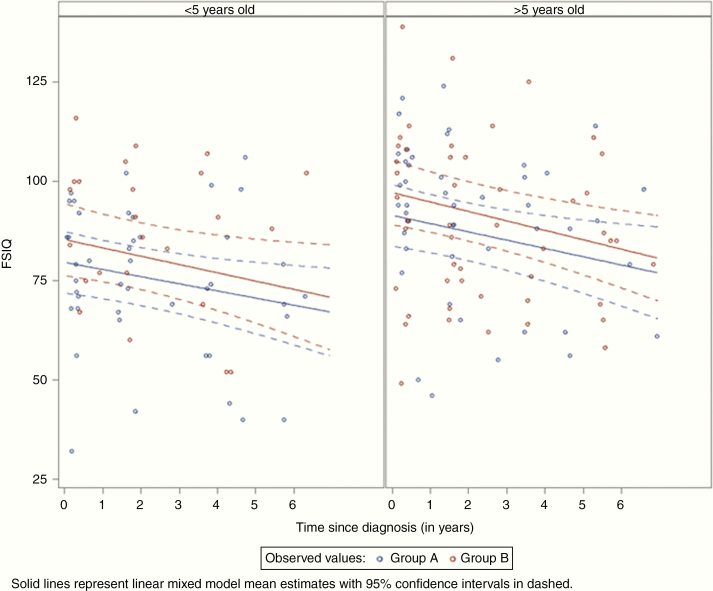
Results: The rate of complete tumor excision was significantly higher in group B than in group A (93.3% vs 57.4%, P = 0.0013). Postoperative complications, chemotherapy-associated side effects, and local progressions were not increased in group B. Neoadjuvant chemotherapy led to a decrease in the primary tumor size in all patients; meanwhile 4/38 patients experienced a distant progression. The histological review of 19 matched tumor pairs (before and after chemotherapy) showed that proliferation was reduced and histological diagnosis feasible and accurate even after neoadjuvant chemotherapy. The 5-year progression-free and overall survival rates were comparable between groups. Comparison of the longitudinal neuropsychological data showed that intellectual outcome tended to be better in group B (the mean predicted intellectual quotient value was 6 points higher throughout the follow-up).
Conclusion: Preoperative chemotherapy is a safe and efficient strategy for metastatic medulloblastoma. It increases the rate of complete tumor excision and may improve the neuropsychological outcome without jeopardizing survival.
Key points: 1. Preoperative chemotherapy increases the rate of complete tumor removal.2. No additional risk (toxic or disease progression) is linked to the delayed surgery.3. Preoperative chemotherapy could have a positive impact on the neuropsychological outcome of patients.
Keywords: childhood brain tumor; medulloblastoma; neuropsychological outcome; preoperative chemotherapy; surgery.
© The Author(s) 2020. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Figures
Comment in
-
Preoperative chemotherapy in medulloblastoma: a change in treatment paradigm?Neuro Oncol. 2020 Nov 26;22(11):1562-1563. doi: 10.1093/neuonc/noaa213. Neuro Oncol. 2020. PMID: 32920640 Free PMC article. No abstract available.
References
-
- Albright AL, Wisoff JH, Zeltzer PM, Boyett JM, Rorke LB, Stanley P. Effects of medulloblastoma resections on outcome in children: a report from the Children’s Cancer Group. Neurosurgery. 1996;38(2):265–271. - PubMed
-
- Zeltzer PM, Boyett JM, Finlay JL, et al. Metastasis stage, adjuvant treatment, and residual tumor are prognostic factors for medulloblastoma in children: conclusions from the Children’s Cancer Group 921 randomized phase III study. J Clin Oncol. 1999;17(3):832–845. - PubMed
-
- Massimino M, Antonelli M, Gandola L, et al. Histological variants of medulloblastoma are the most powerful clinical prognostic indicators. Pediatr Blood Cancer. 2013;60(2):210–216. - PubMed
-
- Pfister S, Remke M, Benner A, et al. Outcome prediction in pediatric medulloblastoma based on DNA copy-number aberrations of chromosomes 6q and 17q and the MYC and MYCN loci. J Clin Oncol. 2009;27(10):1627–1636. - PubMed
