

Battling COVID-19: critical care and peri-operative healthcare resource management strategies in a tertiary academic medical centre in Singapore
- PMID: 32267963
- PMCID: PMC7262214
- DOI: 10.1111/anae.15074
Battling COVID-19: critical care and peri-operative healthcare resource management strategies in a tertiary academic medical centre in Singapore
Abstract
In December 2019, a cluster of atypical pneumonia cases were reported in Wuhan, China, and a novel coronavirus elucidated as the aetiologic agent. Although most initial cases occurred in China, the disease, termed coronavirus disease 2019, has become a pandemic and continues to spread rapidly with human-to-human transmission in many countries. This is the third novel coronavirus outbreak in the last two decades and presents an ensuing healthcare resource burden that threatens to overwhelm available healthcare resources. A study of the initial Chinese response has shown that there is a significant positive association between coronavirus disease 2019 mortality and healthcare resource burden. Based on the Chinese experience, some 19% of coronavirus disease 2019 cases develop severe or critical disease. This results in a need for adequate preparation and mobilisation of critical care resources to anticipate and adapt to a surge in coronavirus disease 2019 case-load in order to mitigate morbidity and mortality. In this article, we discuss some of the peri-operative and critical care resource planning considerations and management strategies employed in a tertiary academic medical centre in Singapore in response to the coronavirus disease 2019 outbreak.
Keywords: COVID-19; critical care; healthcare; peri-operative; resource management.
© 2020 Association of Anaesthetists.
Figures
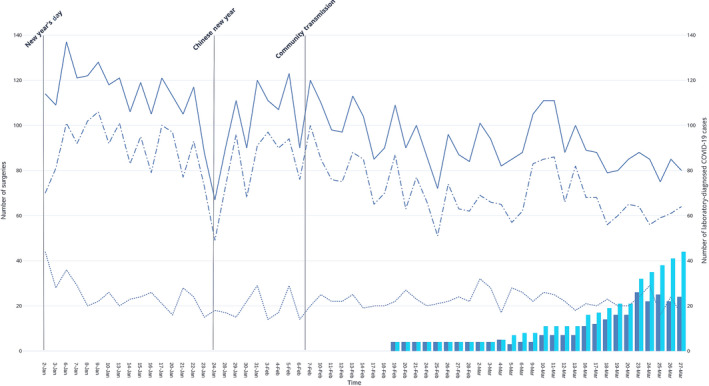
 ) Total surgeries; (
) Total surgeries; ( )Elective surgeries; (
)Elective surgeries; ( )Emergency surgeries; (
)Emergency surgeries; ( ) Admitted COVID‐19 patients; (
) Admitted COVID‐19 patients; ( )Cumulative total COVID‐19 patients.
)Cumulative total COVID‐19 patients.
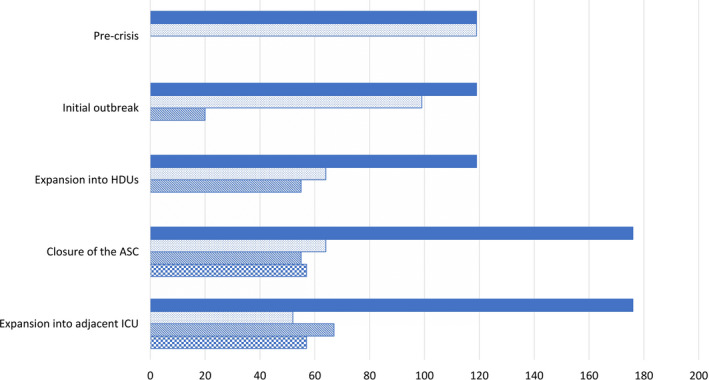
 ) total critical care unit bed space; (
) total critical care unit bed space; ( )clean ICU bed space; (
)clean ICU bed space; ( ) cohort ICU bed space; (
) cohort ICU bed space; ( ) expanded clean HDU bed space.
) expanded clean HDU bed space.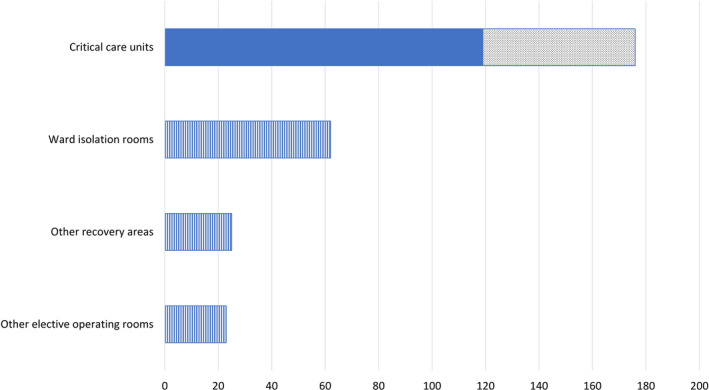
 ) pre‐crisis baseline; (
) pre‐crisis baseline; ( )additional critical care unit bed space; (
)additional critical care unit bed space; ( ) additional facilities that may be utilised.
) additional facilities that may be utilised.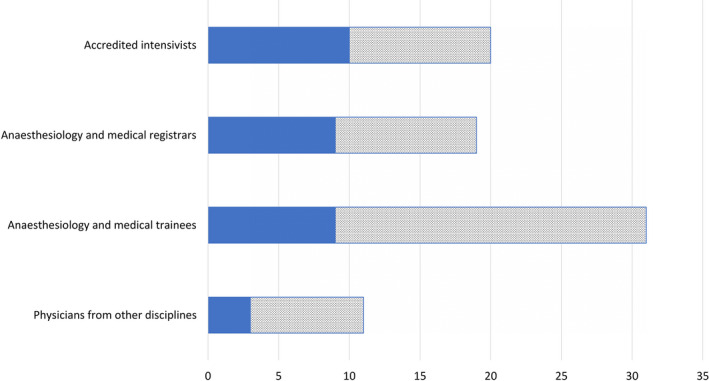
 ) pre‐crisis physician manpower; (
) pre‐crisis physician manpower; ( )projected physician manpower.
)projected physician manpower.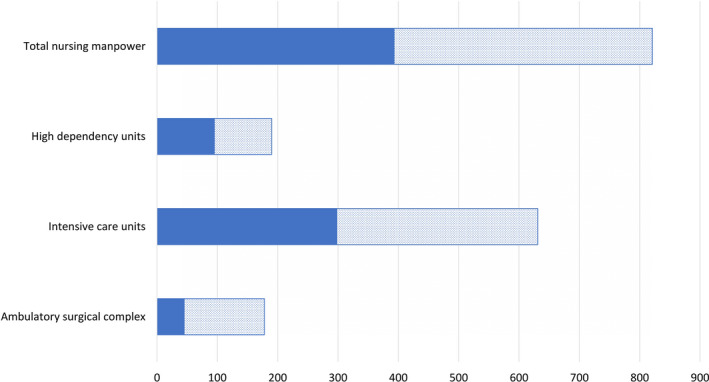
 ) pre‐crisis nursing manpower; (
) pre‐crisis nursing manpower; ( ) projected nursing manpower.
) projected nursing manpower.References
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID‐19) outbreak in china: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. Journal of the American Medical Association 2020. Epub 24 February. 10.1001/jama.2020.2648 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
