

Risk assessment of endometrial cancer and endometrial intraepithelial neoplasia in women with abnormal bleeding and implications for clinical management algorithms
- PMID: 32268124
- PMCID: PMC7529796
- DOI: 10.1016/j.ajog.2020.03.032
Risk assessment of endometrial cancer and endometrial intraepithelial neoplasia in women with abnormal bleeding and implications for clinical management algorithms
Abstract
Background: Most endometrial cancer cases are preceded by abnormal uterine bleeding, offering a potential opportunity for early detection and cure of endometrial cancer. Although clinical guidelines exist for diagnostic workup of abnormal uterine bleeding, consensus is lacking regarding optimal management for women with abnormal bleeding to diagnose endometrial cancer.
Objective: We report the baseline data from a prospective clinical cohort study of women referred for endometrial evaluation at the Mayo Clinic, designed to evaluate risk stratification in women at increased risk for endometrial cancer. Here, we introduce a risk-based approach to evaluate diagnostic tests and clinical management algorithms in a population of women with abnormal bleeding undergoing endometrial evaluation at the Mayo Clinic.
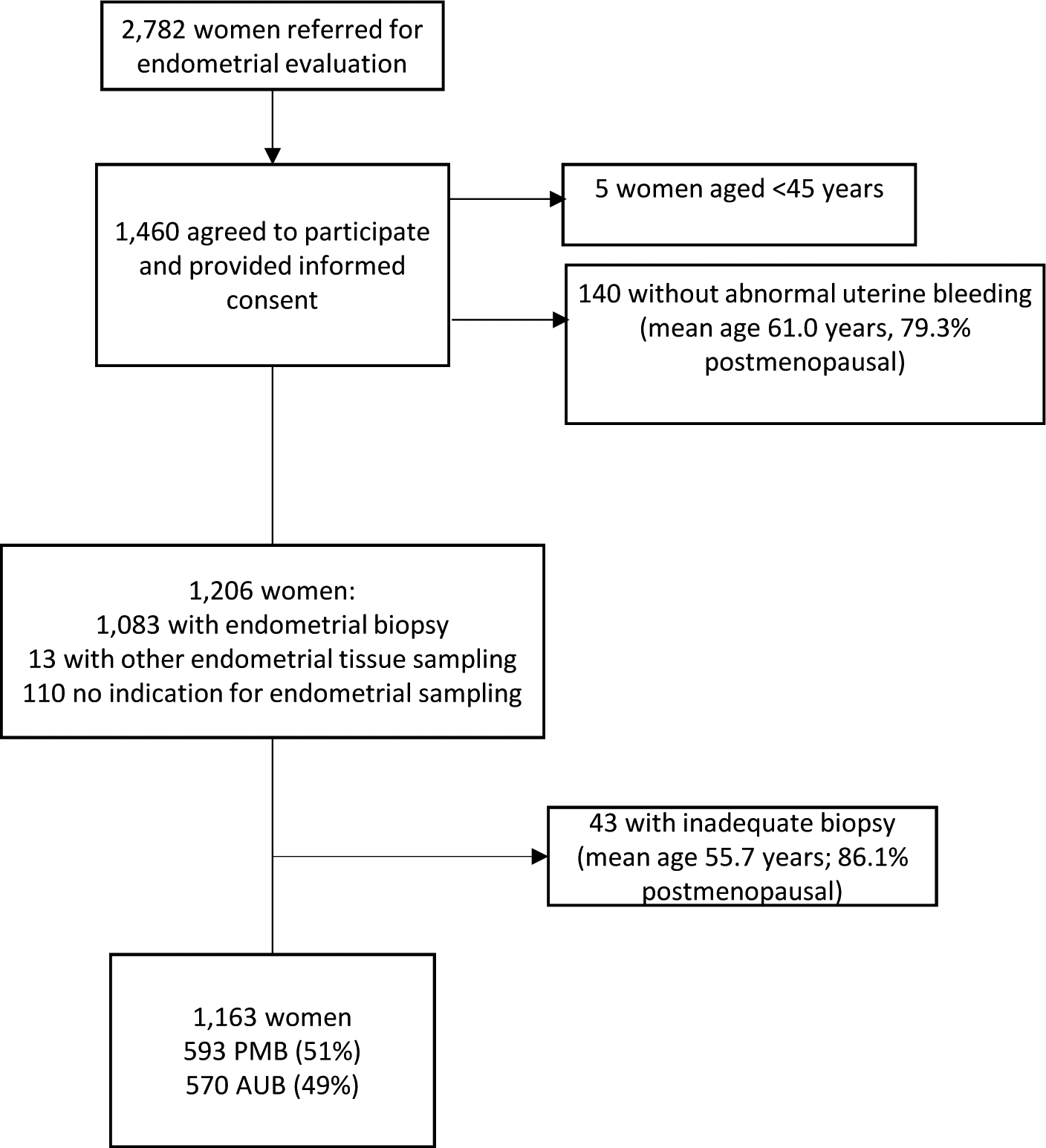
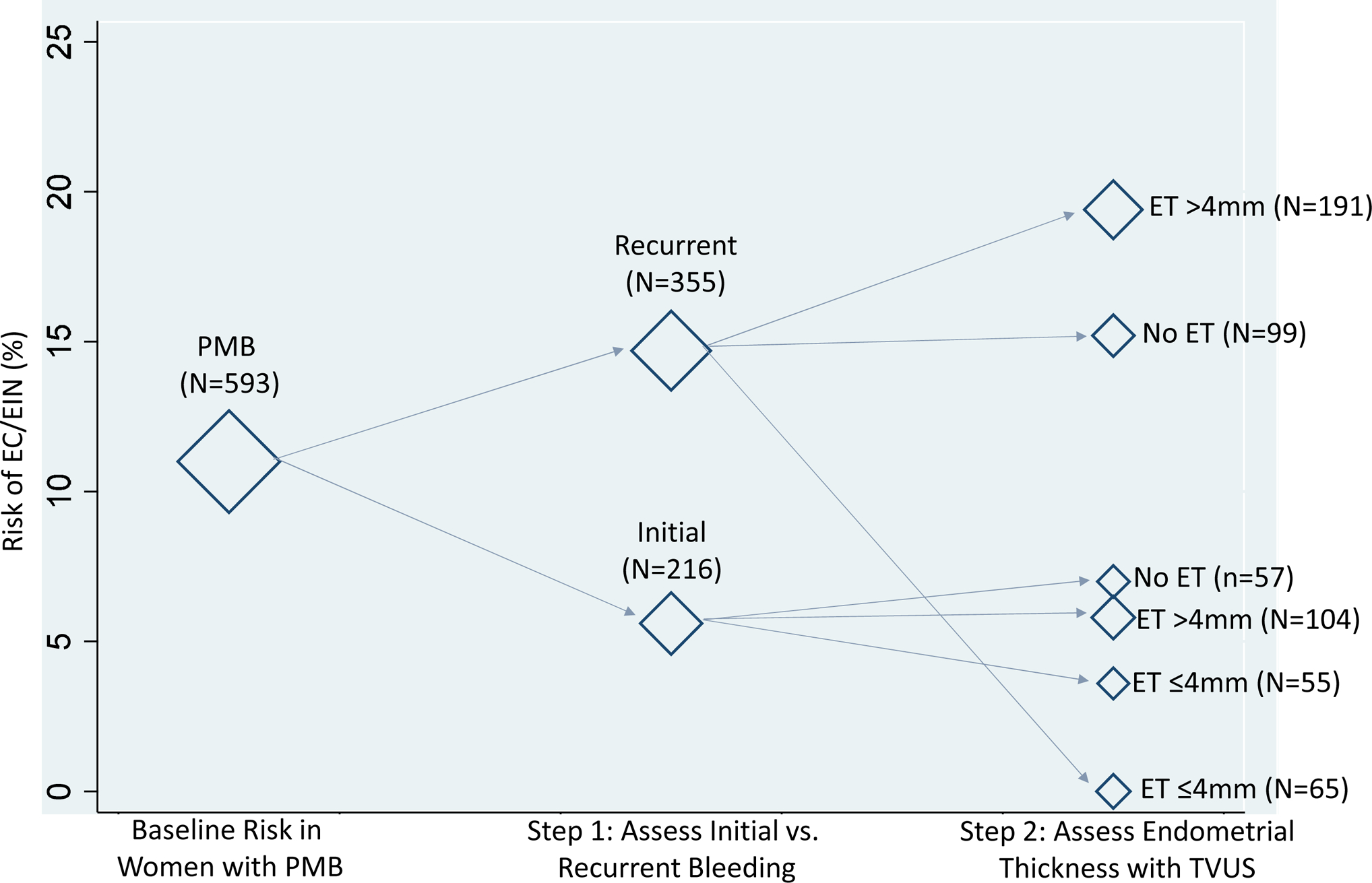
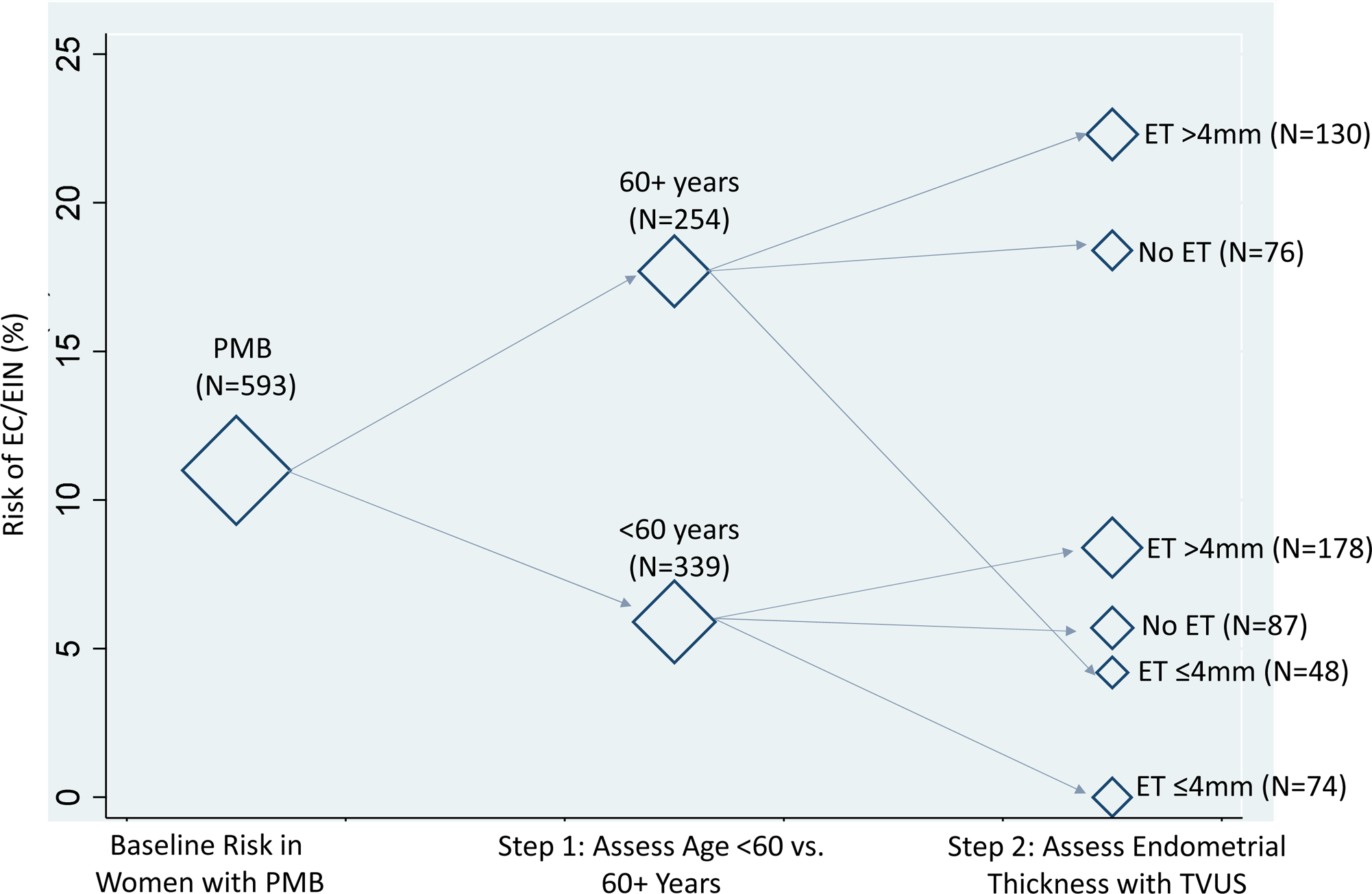
Study design: A total of 1163 women aged ≥45 years were enrolled from February 2013 to May 2019. We evaluated baseline absolute risks and 95% confidence intervals of endometrial cancer and endometrial intraepithelial neoplasia according to clinical algorithms for diagnostic workup of women with postmenopausal bleeding (assessment of initial vs recurrent bleeding episode and endometrial thickness measured through transvaginal ultrasound). We also evaluated risks among women with postmenopausal bleeding according to baseline age (<60 vs 60+ years) as an alternative example. For this approach, biopsy would be conducted for all women aged 60+ years and those aged <60 years with an endometrial thickness of >4 mm. We assessed the clinical efficiency of each strategy by estimating the percentage of women who would be referred for endometrial biopsy, the percentage of cases detected and missed, and the ratio of biopsies per case detected.
Results: Among the 593 women with postmenopausal bleeding, 18 (3.0%) had endometrial intraepithelial neoplasia, and 47 (7.9%) had endometrial cancer, and among the 570 premenopausal women with abnormal bleeding, 8 (1.4%) had endometrial intraepithelial neoplasia, and 7 (1.2%) had endometrial cancer. Maximum risk was noted in women aged 60+ years (17.7%; 13.0%-22.3%), followed by those with recurrent bleeding (14.7%; 11.0%-18.3%). Among women with an initial bleeding episode for whom transvaginal ultrasound was recommended, endometrial thickness did not provide meaningful risk stratification: risks of endometrial cancer and endometrial intraepithelial neoplasia were nearly identical in women with an endometrial thickness of >4 mm (5.8%; 1.3%-10.3%) and ≤4 mm (3.6%; 0.9%-8.6%). In contrast, among those aged <60 years with an endometrial thickness of >4 mm, the risk of endometrial cancer and endometrial intraepithelial neoplasia was 8.4% (4.3%-12.5%), and in those with an endometrial thickness of ≤4 mm, the risk was 0% (0.0%-3.0%; P=.01). The most efficient strategy was to perform biopsy in all women aged 60+ years and among those aged <60 years with an endometrial thickness of >4 mm, with the lowest percentage referred to biopsy while still detecting all cases.
Conclusion: Existing clinical recommendations for endometrial cancer detection in women with abnormal bleeding are not consistent with the underlying risk. Endometrial cancer risk factors such as age can provide important risk stratification compared with the assessment of recurrent bleeding. Future research will include a formal assessment of clinical and epidemiologic risk prediction models in our study population as well as validation of our findings in other populations.
Keywords: abnormal bleeding; endometrial biopsy; endometrial cancer; endometrial intraepithelial neoplasia; postmenopausal bleeding; risk assessment; transvaginal ultrasound.
Published by Elsevier Inc.
Conflict of interest statement
Figures
Comment in
-
Abnormal uterine bleeding and the risk of endometrial cancer: can subendometrial vascular ultrasound be of help to discriminate cancer from adenomyosis?Am J Obstet Gynecol. 2020 Oct;223(4):605-606. doi: 10.1016/j.ajog.2020.05.049. Epub 2020 Jun 1. Am J Obstet Gynecol. 2020. PMID: 32497607 No abstract available.
-
Excerpts from the World Medical Literature.J Obstet Gynaecol Can. 2021 Mar;43(3):290-293. doi: 10.1016/j.jogc.2020.12.010. J Obstet Gynaecol Can. 2021. PMID: 33640097 No abstract available.
References
-
- Lortet-Tieulent J, Ferlay J, Bray F, Jemal A. International Patterns and Trends in Endometrial Cancer Incidence, 1978–2013. J Natl Cancer Inst. 2017. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34. - PubMed
-
- Weiderpass E, Antoine J, Bray FI, Oh JK, Arbyn M. Trends in corpus uteri cancer mortality in member states of the European Union. Eur J Cancer. 2014;50:1675–84. - PubMed
-
- Creasman WT, Odicino F, Maisonneuve P, Quinn MA, Beller U, Benedet JL, et al. Carcinoma of the corpus uteri. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynaecol Obstet. 2006;95 Suppl 1:S105–43. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
