

Bleeding and response to hemostatic therapy in acquired hemophilia A: results from the GTH-AH 01/2010 study
- PMID: 32268359
- PMCID: PMC7392842
- DOI: 10.1182/blood.2019003639
Bleeding and response to hemostatic therapy in acquired hemophilia A: results from the GTH-AH 01/2010 study
Abstract
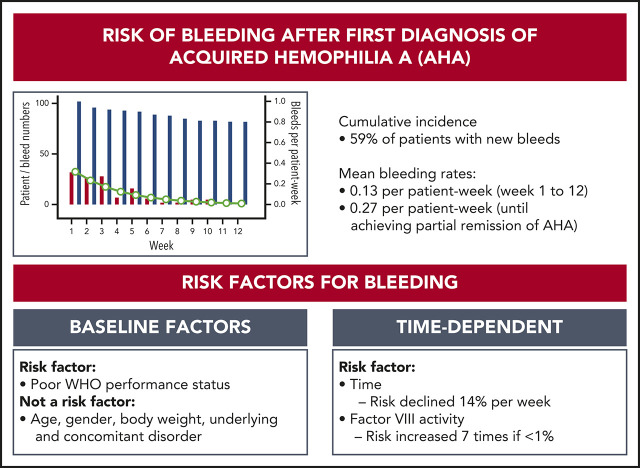
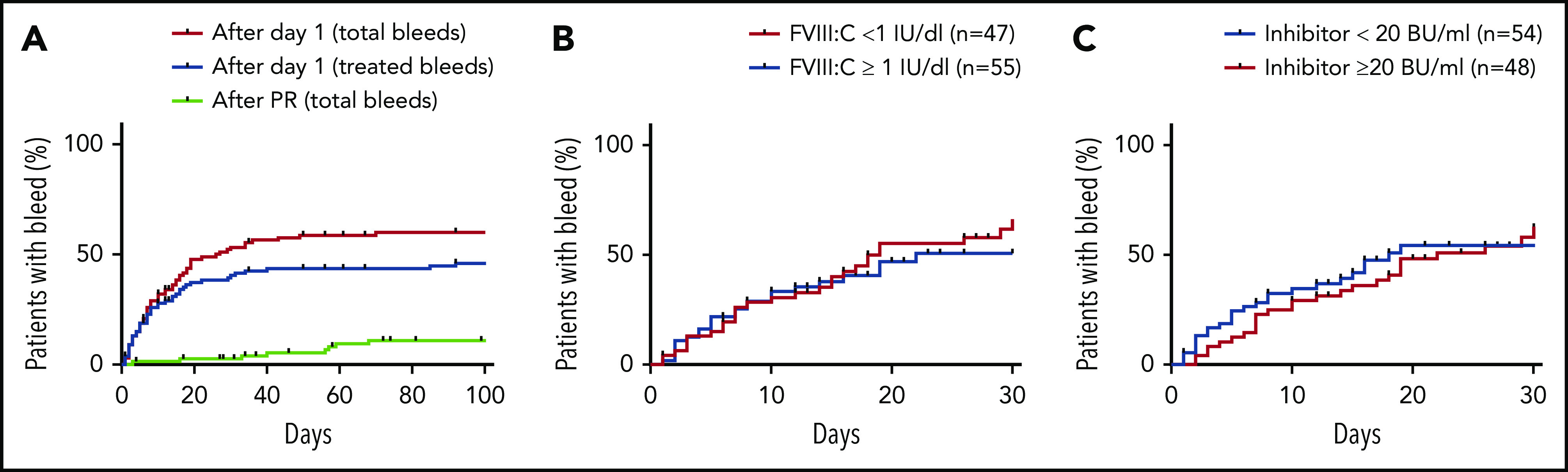
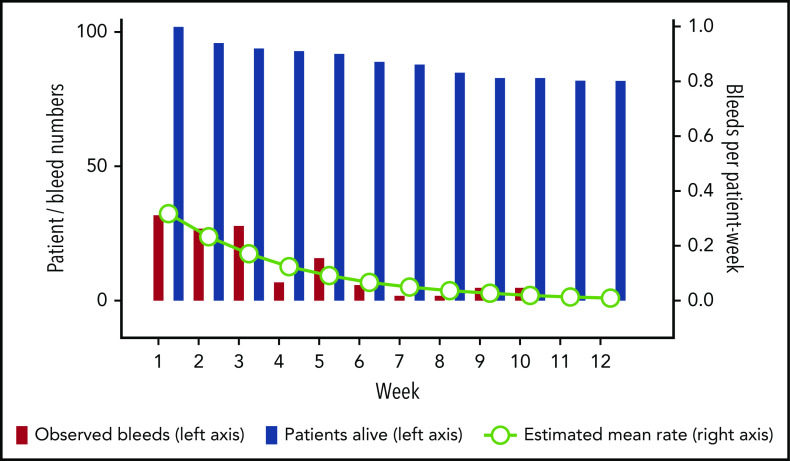
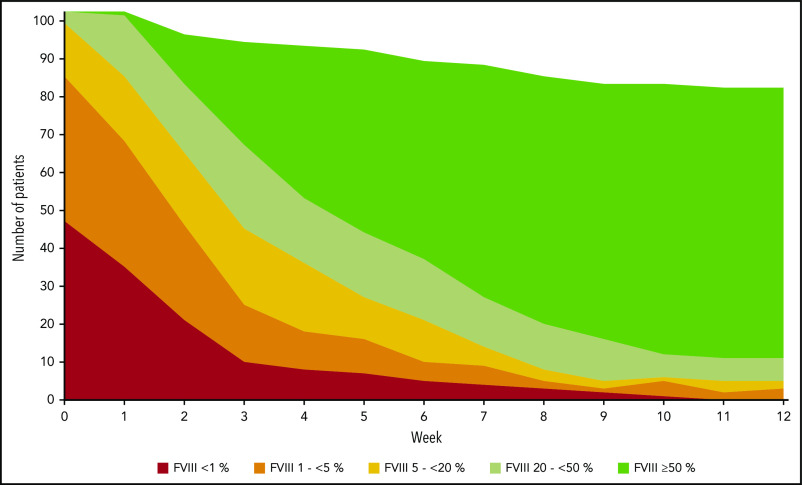
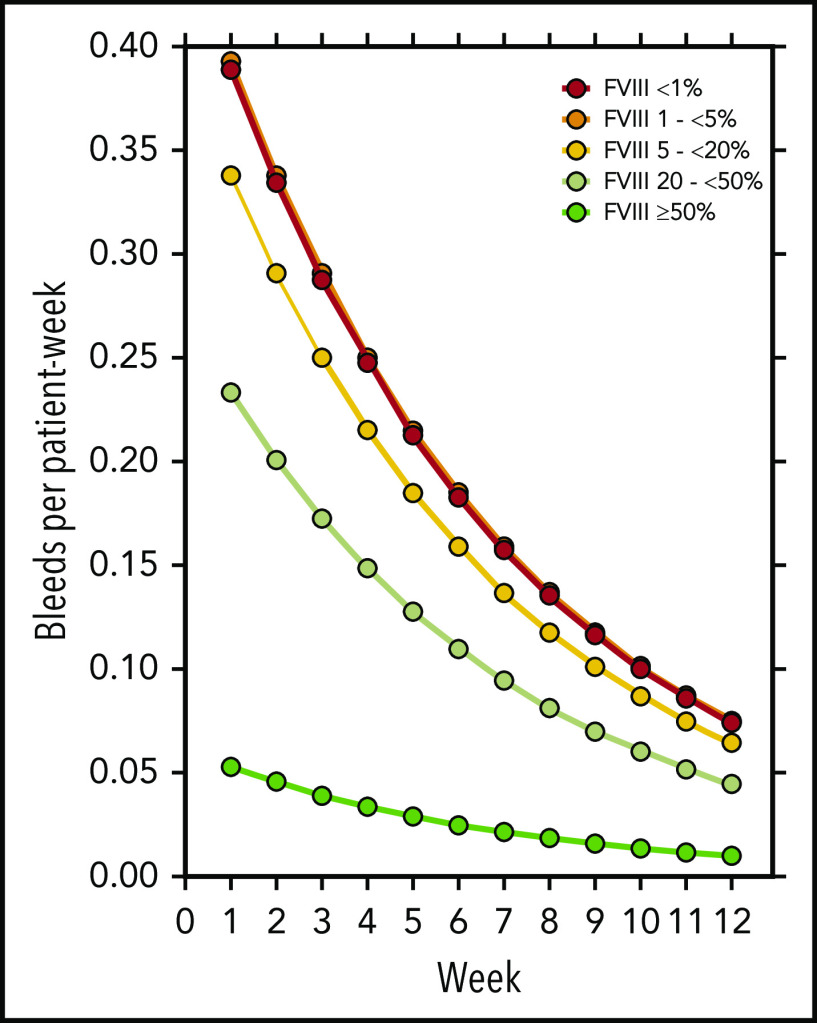
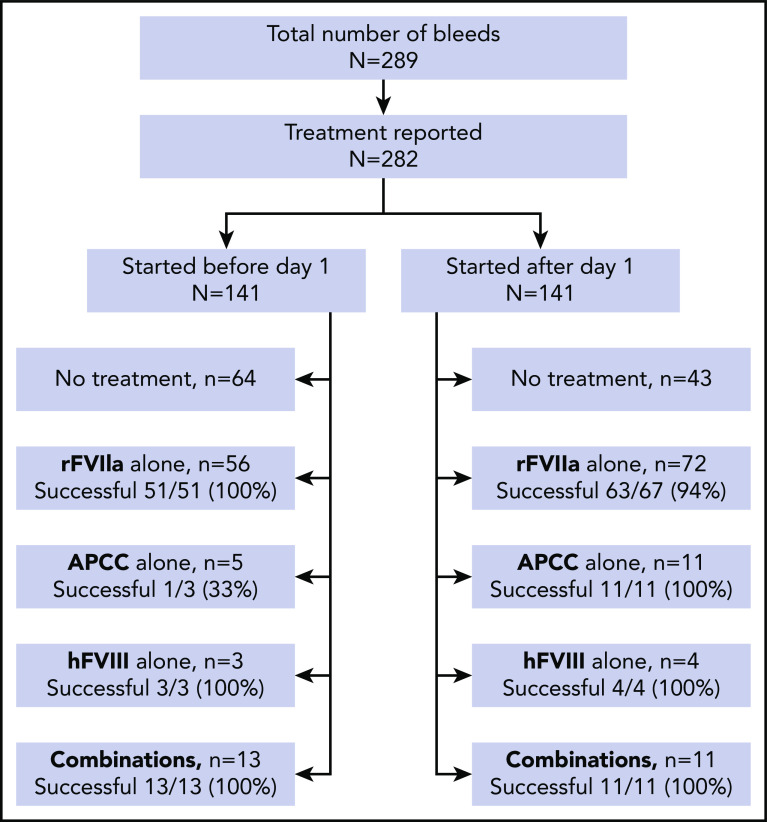
Acquired hemophilia A (AHA) is due to autoantibodies against coagulation factor VIII (FVIII) and most often presents with unexpected bleeding. In contrast to congenital hemophilia, the patient's residual FVIII activity does not seem to correlate with the risk of bleeding as suggested from previous studies. Risk factors for bleeding have not been described. We used data from the prospective GTH-AH 01/2010 study to assess the risk of bleeding and the efficacy of hemostatic therapy. FVIII activity was measured at baseline and weekly thereafter. Bleeding events were assessed by treating physicians. A total of 289 bleeds were recorded in 102 patients. There were 141 new bleeds observed starting after day 1 in 59% of the patients, with a mean rate of 0.13 bleed per patient-week in weeks 1 to 12, or 0.27 bleed per patient-week before achieving partial remission. Weekly measured FVIII activity was significantly associated with the bleeding rate, but only achieving FVIII activity ≥50% abolished the risk of bleeding. A good World Health Organization performance status assessed at baseline (score 0 vs higher) was associated with a lower bleeding rate. Hemostatic treatment was reportedly effective in 96% of bleeds. Thus, the risk of new bleeds after a first diagnosis of AHA remains high until partial remission is achieved, and weekly measured FVIII activity may aid in assessing the individual risk of bleeding. These results will help to define future strategies for prophylaxis of bleeding in AHA.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: K.H. received honoraria for advisory boards or speaker fees from Bayer, Biotest, Chugai, CSL Behring, Novo Nordisk, Pfizer, Roche, Shire/Takeda, and SOBI; and unrestricted research grants from Bayer, CSL Behring, and Pfizer. P.K. received honoraria, consultation and speaker fees, and research and travel grants from Biotest, CSL Behring, Novo Nordisk, Octapharma, Roche, Sanofi, and Baxalta/Shire/Takeda. R.K. received research funding and honoraria from Bayer, BioMarin, Biotest, CSL Behring, Novo Nordisk, Octapharma, Pfizer, Roche, Sanofi, SOBI, and Takeda. U.G. received honoraria for advisory boards and travel grants from Roche, Bayer, and Baxalta/Shire/Takeda. H.E. received honoraria or consultation fees, advisory boards or speaker fees, and research grants from Bayer, Biotest, CSL Behring, Novo Nordisk, Pfizer, Roche, Shire, and SOBI. W.M. received honoraria, research grants, and consultation fees for participating at educational meetings organized by Alnylam, Bayer, Biogen Idec, Biotest, Chugai, CSL Behring, Novo Nordisk, Octapharma, Pfizer, Roche, Shire, and SOBI. A.T. received honoraria or consultation fees for participating at educational meetings organized by Alnylam, Bayer, Biogen Idec, Biotest, Boehringer Ingelheim, Chugai, CSL Behring, Daiichi Sankyo, Leo Pharma, Novo Nordisk, Octapharma, Pfizer, Portola, Roche, Shire, and SOBI. The remaining authors declare no competing financial interests.
Figures
Comment in
-
Bleeding in acquired hemophilia: have we figured it out?Blood. 2020 Jul 16;136(3):262-264. doi: 10.1182/blood.2020006098. Blood. 2020. PMID: 32673389 No abstract available.
References
-
- Kruse-Jarres R, Kempton CL, Baudo F, et al. Acquired hemophilia A: updated review of evidence and treatment guidance. Am J Hematol. 2017;92(7):695-705. - PubMed
-
- Franchini M, Vaglio S, Marano G, et al. Acquired hemophilia A: a review of recent data and new therapeutic options. Hematology. 2017;22(9):514-520. - PubMed
-
- Tiede A, Scharf RE, Dobbelstein C, Werwitzke S. Management of acquired haemophilia A. Hamostaseologie. 2015;35(4):311-318. - PubMed
-
- Collins PW, Hirsch S, Baglin TP, et al. ; UK Haemophilia Centre Doctors’ Organisation . Acquired hemophilia A in the United Kingdom: a 2-year national surveillance study by the United Kingdom Haemophilia Centre Doctors’ Organisation. Blood. 2007;109(5):1870-1877. - PubMed
-
- Knoebl P, Marco P, Baudo F, et al. ; EACH2 Registry Contributors . Demographic and clinical data in acquired hemophilia A: results from the European Acquired Haemophilia Registry (EACH2). J Thromb Haemost. 2012;10(4):622-631. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
