

Projecting demand for critical care beds during COVID-19 outbreaks in Canada
- PMID: 32269020
- PMCID: PMC7234264
- DOI: 10.1503/cmaj.200457
Projecting demand for critical care beds during COVID-19 outbreaks in Canada
Abstract
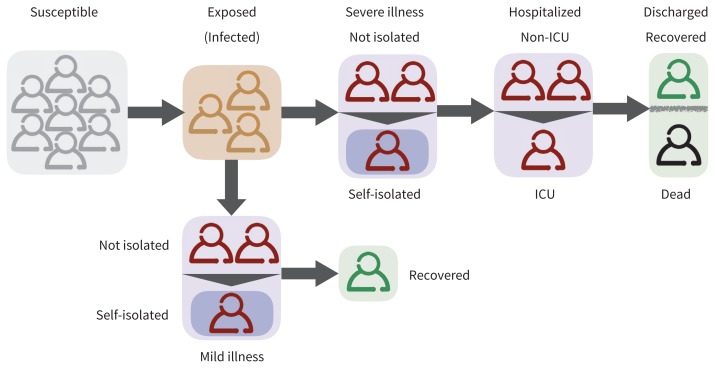
Background: Increasing numbers of coronavirus disease 2019 (COVID-19) cases in Canada may create substantial demand for hospital admission and critical care. We evaluated the extent to which self-isolation of mildly ill people delays the peak of outbreaks and reduces the need for this care in each Canadian province.
Methods: We developed a computational model and simulated scenarios for COVID-19 outbreaks within each province. Using estimates of COVID-19 characteristics, we projected the hospital and intensive care unit (ICU) bed requirements without self-isolation, assuming an average number of 2.5 secondary cases, and compared scenarios in which different proportions of mildly ill people practised self-isolation 24 hours after symptom onset.
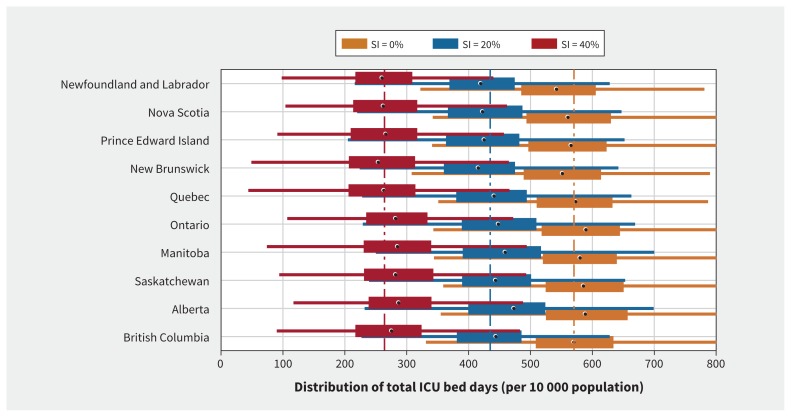
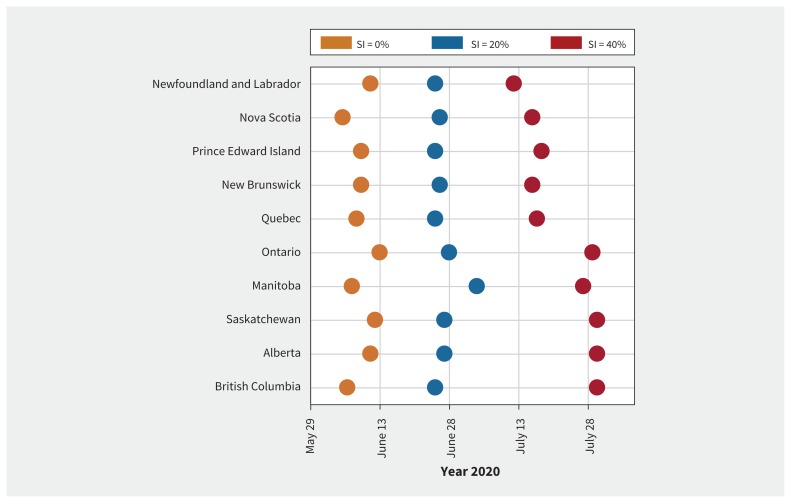
Results: Without self-isolation, the peak of outbreaks would occur in the first half of June, and an average of 569 ICU bed days per 10 000 population would be needed. When 20% of cases practised self-isolation, the peak was delayed by 2-4 weeks, and ICU bed requirement was reduced by 23.5% compared with no self-isolation. Increasing self-isolation to 40% reduced ICU use by 53.6% and delayed the peak of infection by an additional 2-4 weeks. Assuming current ICU bed occupancy rates above 80% and self-isolation of 40%, demand would still exceed available (unoccupied) ICU bed capacity.
Interpretation: At the peak of COVID-19 outbreaks, the need for ICU beds will exceed the total number of ICU beds even with self-isolation at 40%. Our results show the coming challenge for the health care system in Canada and the potential role of self-isolation in reducing demand for hospital-based and ICU care.
© 2020 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Joanne Langley reports that Dalhousie University has received payment for conduct of vaccine studies from Sanofi, Glaxo-SmithKline, Merck, Janssen, VBI and Pfizer. Dr. Langley holds the Canadian Institutes of Health Research-GlaxoSmithKline Chair in Pediatric Vaccinology. No other competing interests were declared.
Figures
Comment in
-
Social distancing to combat COVID-19: We are all on the front line.CMAJ. 2020 May 11;192(19):E516-E517. doi: 10.1503/cmaj.200606. Epub 2020 Apr 8. CMAJ. 2020. PMID: 32269019 Free PMC article. No abstract available.
References
-
- Coronavirus COVID-19 global cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Johns Hopkins Coronavirus Resource Center; Available: www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e... (accessed 2020 Mar. 19).
-
- Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 2020. Feb. 24pii S2213-2600(20)30079-5 [Epub ahead of print]. 10.1016/S2213-2600(20)30079-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical