

Impact of Neoadjuvant Durvalumab with or without Tremelimumab on CD8+ Tumor Lymphocyte Density, Safety, and Efficacy in Patients with Oropharynx Cancer: CIAO Trial Results
- PMID: 32269052
- PMCID: PMC8362306
- DOI: 10.1158/1078-0432.CCR-19-3977
Impact of Neoadjuvant Durvalumab with or without Tremelimumab on CD8+ Tumor Lymphocyte Density, Safety, and Efficacy in Patients with Oropharynx Cancer: CIAO Trial Results
Abstract
Purpose: In oropharyngeal squamous cell carcinoma (OPC), high CD8+ tumor-infiltrating lymphocyte (CD8+TIL) density confers improved prognosis. We compared neoadjuvant durvalumab (PD-L1 inhibitor) with durvalumab + tremelimumab (CTLA-4 inhibitor) in terms of impact on CD8+TIL density, safety, and efficacy in patients with OPC.
Patients and methods: Patients with newly diagnosed stage II-IVA OPC or locoregionally recurrent OPC amenable to resection were included. Patients were randomized to two cycles of durvalumab or durvalumab + tremelimumab before surgery. The primary endpoint was change between baseline and resection specimen in CD8+TIL density between arms. Secondary endpoints included safety, response rate per RECIST, major pathologic response (MPR; ≤10% viable tumor cells) rate, and patient-reported outcomes.
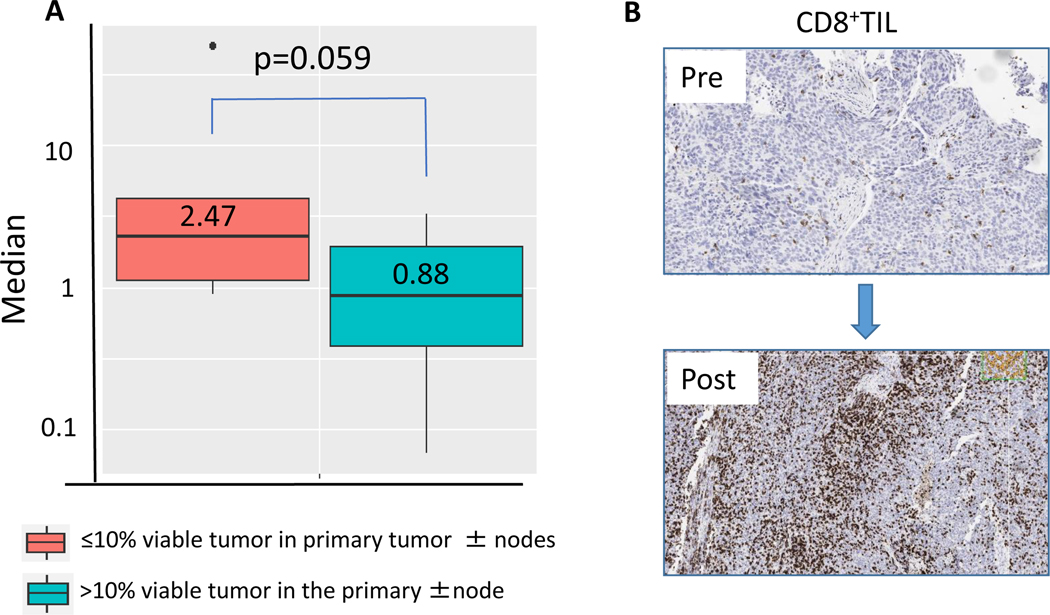
Results: Of 28 eligible patients (14/arm), 20 (71%) had newly diagnosed OPC, and 24 (86%) were p16-positive. The posttreatment to pretreatment median CD8+TIL density ratio was 1.31 for durvalumab and 1.15 for combination treatment (P = 0.97; 95% CI: -1.07-2.28). In each group, 6 patients (43%, 95% CI: 17.66-71.14) had a response. Eight patients (29%) had a MPR at the primary tumor and/or nodal metastases. Neither baseline CD8+TIL density nor PD-L1 expression level correlated with overall response, but a trend toward greater CD8+TIL change in patients with a MPR was seen (P = 0.059; 95% CI: -0.33-3.46). Four patients (14%) had grade ≥3 adverse events. At median follow-up time of 15.79 months, all patients were alive, and one had an additional recurrence.
Conclusions: Durvalumab + tremelimumab did not increase CD8+TIL density more than durvalumab alone did. The observed safety and activity support further investigation of neoadjuvant checkpoint inhibitor for OPC.
Trial registration: ClinicalTrials.gov NCT03144778.
©2020 American Association for Cancer Research.
Figures



References
-
- Nguyen-Tan PF, Zhang Q, Ang KK, Weber RS, Rosenthal DI, Soulieres D, et al. Randomized phase III trial to test accelerated versus standard fractionation in combination with concurrent cisplatin for head and neck carcinomas in the Radiation Therapy Oncology Group 0129 trial: long-term report of efficacy and toxicity. J Clin Oncol 2014;32(34):3858–66 doi 10.1200/JCO.2014.55.3925. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
