

Clinical and MRI phenotypes of sarcoidosis-associated myelopathy
- PMID: 32269072
- PMCID: PMC7176244
- DOI: 10.1212/NXI.0000000000000722
Clinical and MRI phenotypes of sarcoidosis-associated myelopathy
Abstract
Objective: To determine the characteristic clinical and spinal MRI phenotypes of sarcoidosis-associated myelopathy (SAM), we analyzed a large cohort of patients with this disorder.
Methods: Patients diagnosed with SAM at a single center between 2000 and 2018 who met the established criteria for definite and probable neurosarcoidosis were included in a retrospective analysis to identify clinical profiles, CSF characteristics, and MRI lesion morphology.
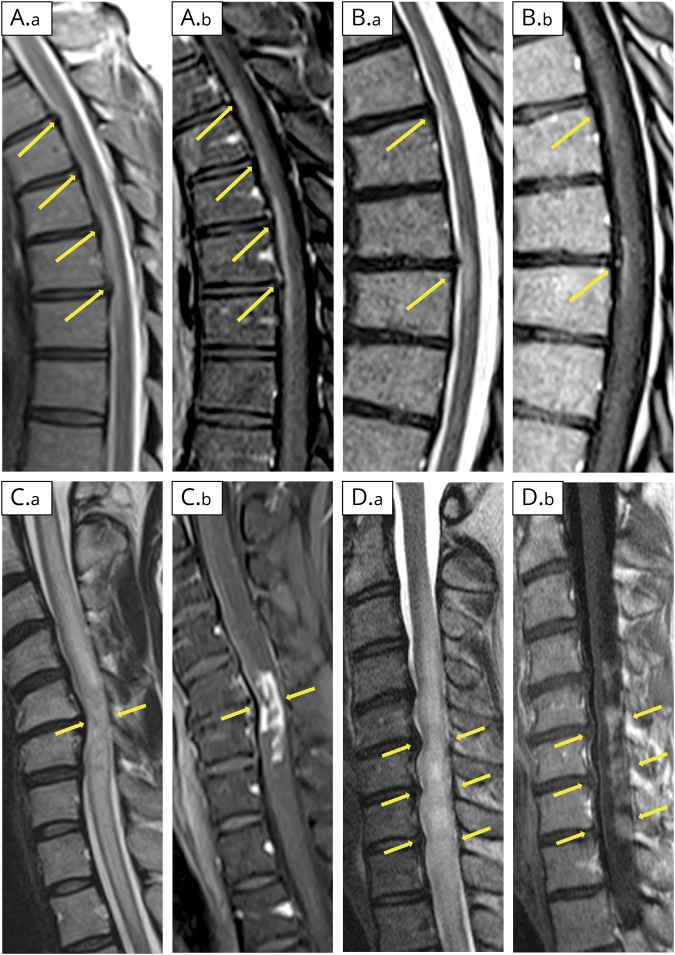
Results: Of 62 included patients, 33 (53%) were male, and 30 (48%) were African American. SAM was the first clinical presentation of sarcoidosis in 49 patients (79%). Temporal profile of symptom evolution was chronic in 81%, with sensory symptoms most frequently reported (87%). CSF studies showed pleocytosis in 79% and CSF-restricted oligoclonal bands in 23% of samples tested. Four discrete patterns of lesion morphology were identified on spine MRI: longitudinally extensive myelitis (n = 28, 45%), short tumefactive myelitis (n = 14, 23%), spinal meningitis/meningoradiculitis (n = 14, 23%), and anterior myelitis associated with areas of disc degeneration (n = 6, 10%). Postgadolinium enhancement was seen in all but 1 patient during the acute phase. The most frequent enhancement pattern was dorsal subpial enhancement (n = 40), followed by meningeal/radicular enhancement (n = 23) and ventral subpial enhancement (n = 12). In 26 cases (42%), enhancement occurred at locations with coexisting structural changes (e.g., spondylosis).
Conclusions: Recognition of the clinical features (chronically evolving myelopathy) and distinct MRI phenotypes (with enhancement in a subpial and/or meningeal pattern) seen in SAM can aid diagnosis of this disorder. Enhancement patterns suggest that SAM may have a predilection for areas of the spinal cord susceptible to mechanical stress.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures


References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous