

Neoadjuvant PROSTVAC prior to radical prostatectomy enhances T-cell infiltration into the tumor immune microenvironment in men with prostate cancer
- PMID: 32269146
- PMCID: PMC7174144
- DOI: 10.1136/jitc-2020-000655
Neoadjuvant PROSTVAC prior to radical prostatectomy enhances T-cell infiltration into the tumor immune microenvironment in men with prostate cancer
Abstract
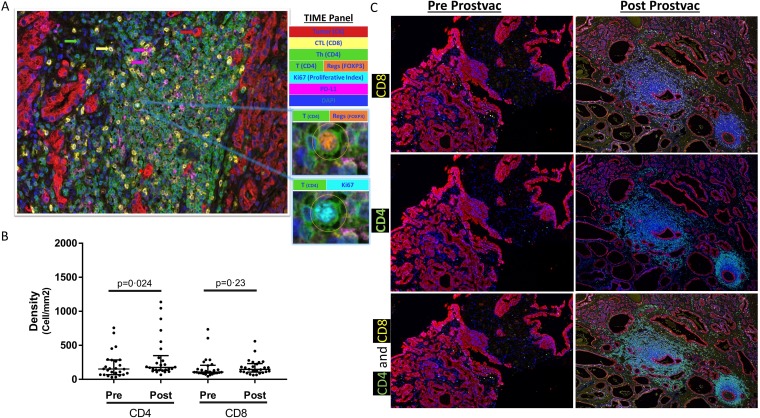
Background: Clinical trials have shown the ability of therapeutic vaccines to generate immune responses to tumor-associated antigens (TAAs). What is relatively less known is if this translates into immune-cell (IC) infiltration into the tumor microenvironment. This study examined whether neoadjuvant prostate-specific antigen (PSA)-targeted vaccination with PROSTVAC could induce T-cell immunity, particularly at the tumor site.
Methods: An open-label, phase II study of neoadjuvant PROSTVAC vaccine enrolled 27 patients with localized prostate cancer awaiting radical prostatectomy (RP). We evaluated increases in CD4 and CD8 T-cell infiltrates (RP tissue vs baseline biopsies) using a six-color multiplex immunofluorescence Opal method. Antigen-specific responses were assessed by intracellular cytokine staining after in vitro stimulation of peripheral blood mononuclear cells with overlapping 15-mer peptide pools encoding the TAAs PSA, brachyury and MUC-1.
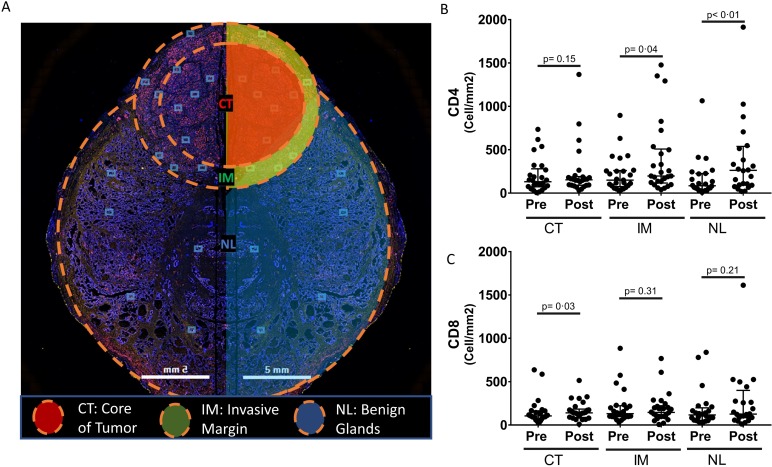
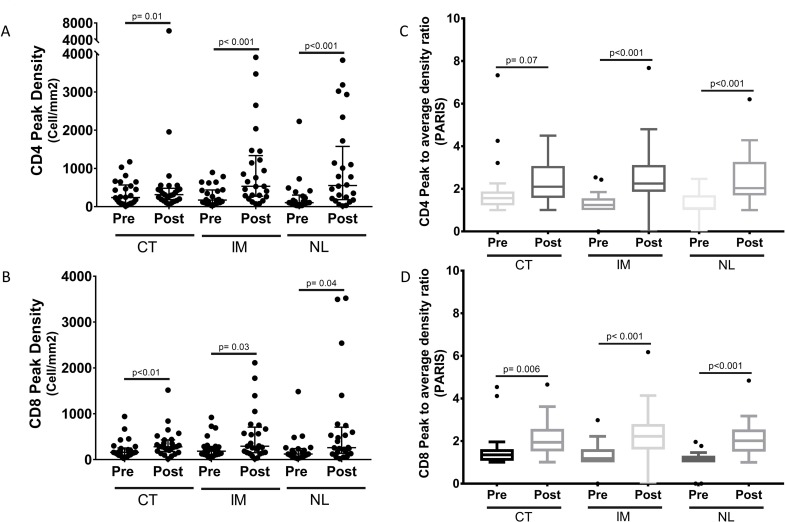
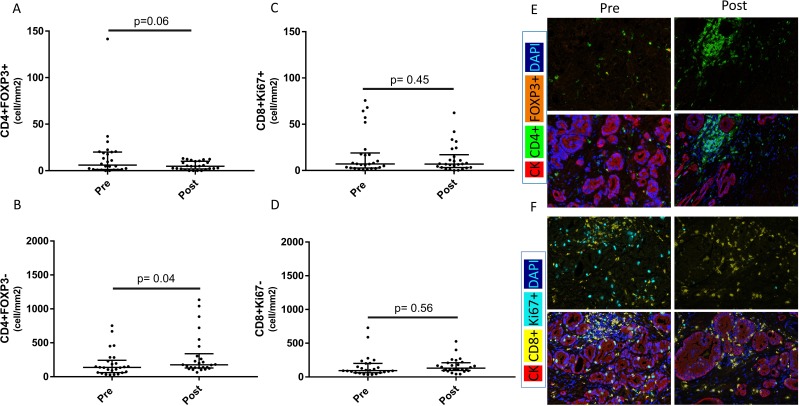
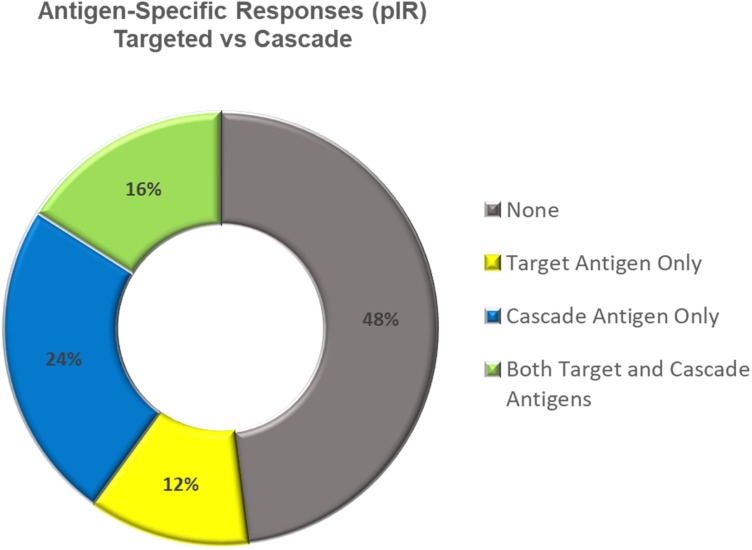
Results: Of 27 vaccinated patients, 26 had matched prevaccination (biopsy) and postvaccination (RP) prostate samples available for non-compartmentalized analysis (NCA) and compartmentalized analysis (CA). Tumor CD4 T-cell infiltrates were significantly increased in postvaccination RP specimens compared with baseline biopsies by NCA (median 176/mm² vs 152/mm²; IQR 136-317/mm² vs 69-284/mm²; p=0.0249; median ratio 1.20; IQR 0.64-2.25). By CA, an increase in both CD4 T-cell infiltrates at the tumor infiltrative margin (median 198/mm² vs 151/mm²; IQR 123-500/mm² vs 85-256/mm²; p=0.042; median ratio 1.44; IQR 0.59-4.17) and in CD8 T-cell infiltrates at the tumor core (median 140/mm² vs 105/mm²; IQR 91-175/mm² vs 83-163/mm²; p=0.036; median ratio 1.25; IQR 0.88-2.09) were noted in postvaccination RP specimens compared with baseline biopsies. A total of 13/25 patients (52%) developed peripheral T-cell responses to any of the three tested TAAs (non-neoantigens); five of these had responses to more than one antigen of the three evaluated.
Conclusion: Neoadjuvant PROSTVAC can induce both tumor immune response and peripheral immune response.
Trial registration number: NCT02153918.
Keywords: clinical trials as topic; immunotherapy, active; tumor microenvironment; urologic neoplasms; vaccination.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: The NCI has a collaborative research and development agreement (CRADA) with Bavarian Nordic, the manufacturer of the vaccine used in this study. Under this CRADA, resources to develop agents are provided, including the vaccine.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous