

Emerging concepts in ventilation-induced lung injury
- PMID: 32269759
- PMCID: PMC7111496
- DOI: 10.12688/f1000research.20576.1
Emerging concepts in ventilation-induced lung injury
Abstract
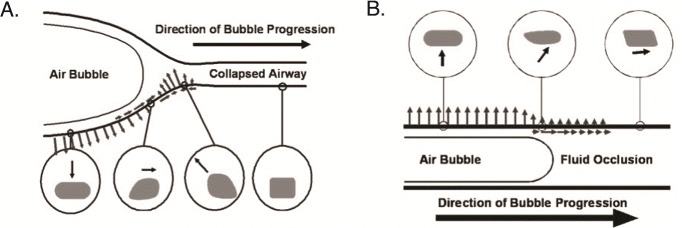
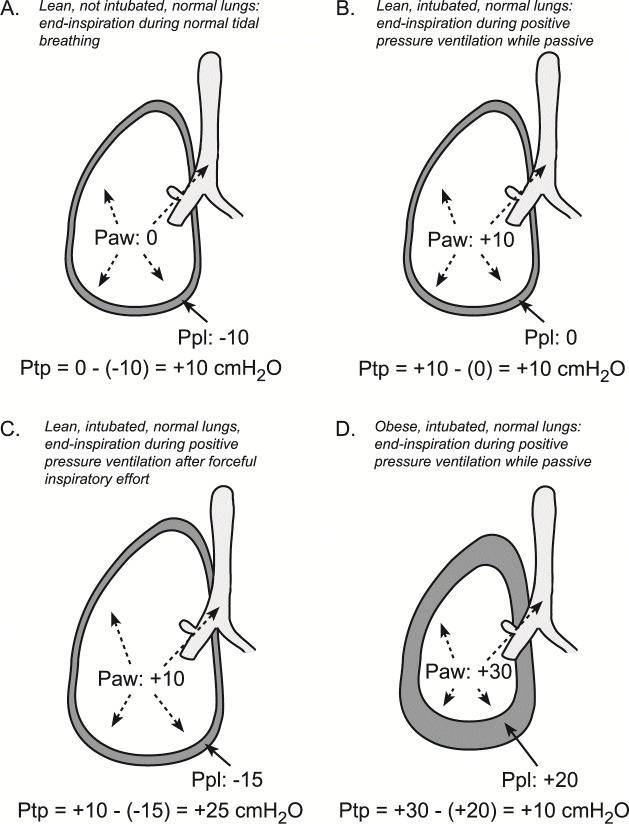
Ventilation-induced lung injury results from mechanical stress and strain that occur during tidal ventilation in the susceptible lung. Classical descriptions of ventilation-induced lung injury have focused on harm from positive pressure ventilation. However, injurious forces also can be generated by patient effort and patient-ventilator interactions. While the role of global mechanics has long been recognized, regional mechanical heterogeneity within the lungs also appears to be an important factor propagating clinically significant lung injury. The resulting clinical phenotype includes worsening lung injury and a systemic inflammatory response that drives extrapulmonary organ failures. Bedside recognition of ventilation-induced lung injury requires a high degree of clinical acuity given its indistinct presentation and lack of definitive diagnostics. Yet the clinical importance of ventilation-induced lung injury is clear. Preventing such biophysical injury remains the most effective management strategy to decrease morbidity and mortality in patients with acute respiratory distress syndrome and likely benefits others at risk.
Keywords: acute lung injury; acute respiratory distress syndrome; mechanical ventilation; respiratory mechanics; ventilator-induced lung injury.
Copyright: © 2020 Madahar P and Beitler JR.
Conflict of interest statement
No competing interests were disclosed.No competing interests were disclosed.No competing interests were disclosed.No competing interests were disclosed.No competing interests were disclosed.
Figures
References
-
- Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, et al. : Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–8. 10.1056/NEJM200005043421801 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources