

Quantifying systemic congestion with Point-Of-Care ultrasound: development of the venous excess ultrasound grading system
- PMID: 32270297
- PMCID: PMC7142196
- DOI: 10.1186/s13089-020-00163-w
Quantifying systemic congestion with Point-Of-Care ultrasound: development of the venous excess ultrasound grading system
Abstract
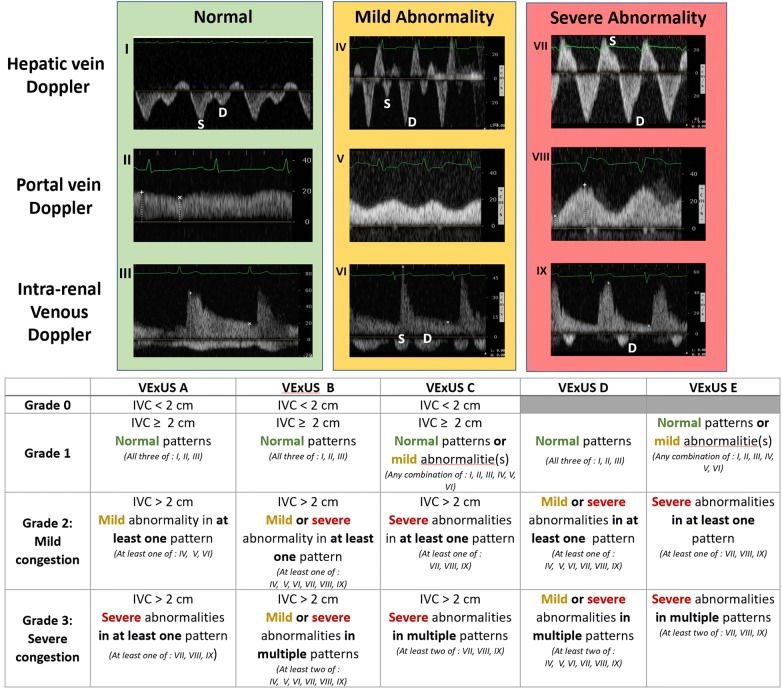
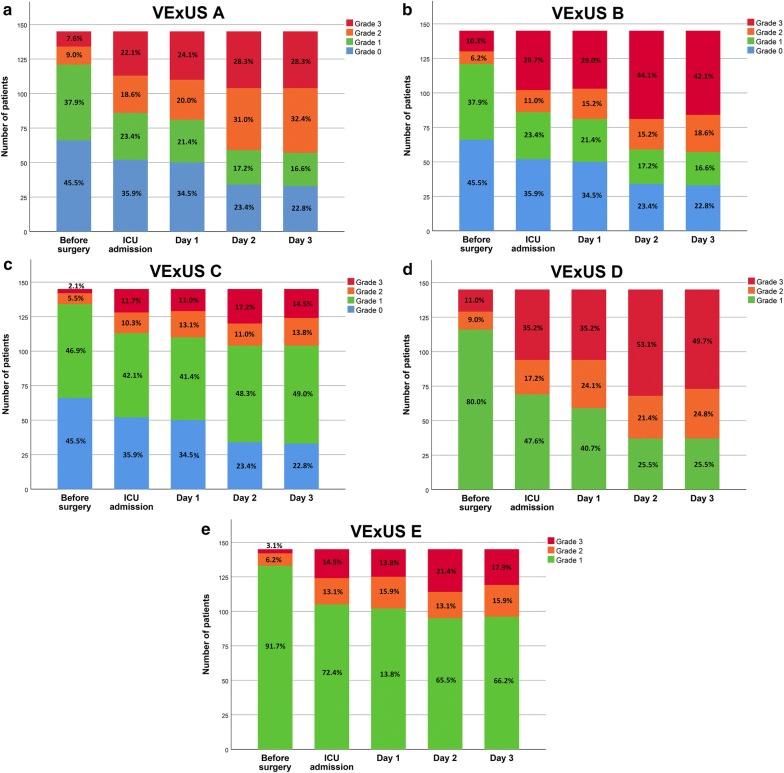
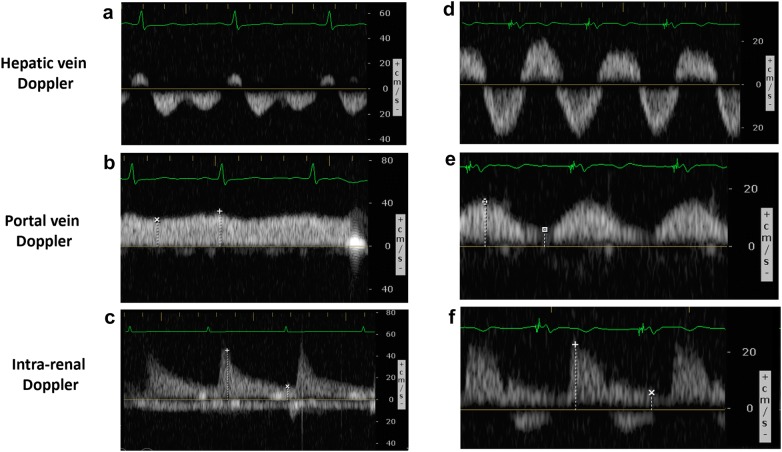
Background: Organ congestion is a mediator of adverse outcomes in critically ill patients. Point-Of-Care ultrasound (POCUS) is widely available and could enable clinicians to detect signs of venous congestion at the bedside. The aim of this study was to develop several grading system prototypes using POCUS and to determine their respective ability to predict acute kidney injury (AKI) after cardiac surgery. This is a post-hoc analysis of a single-center prospective study in 145 patients undergoing cardiac surgery for which repeated daily measurements of hepatic, portal, intra-renal vein Doppler and inferior vena cava (IVC) ultrasound were performed during the first 72 h after surgery. Five prototypes of venous excess ultrasound (VExUS) grading system combining multiple ultrasound markers were developed.
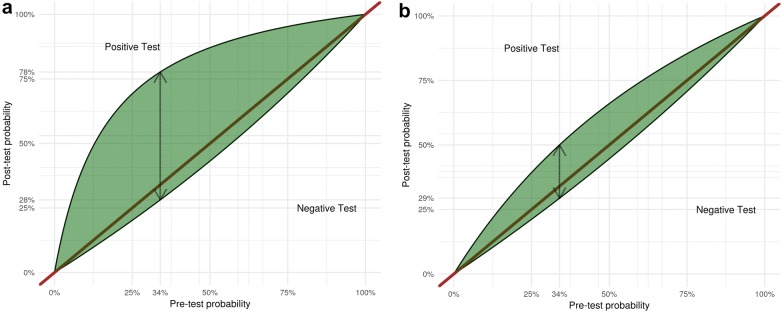
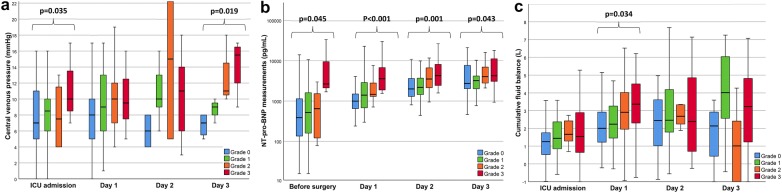
Results: The association between each score and AKI was assessed using time-dependant Cox models as well as conventional performance measures of diagnostic testing. A total of 706 ultrasound assessments were analyzed. We found that defining severe venous congestion as the presence of severe flow abnormalities in multiple Doppler patterns with a dilated IVC (≥ 2 cm) showed the strongest association with the development of subsequent AKI compared with other combinations (HR: 3.69 CI 1.65-8.24 p = 0.001). The association remained significant after adjustment for baseline risk of AKI and vasopressor/inotropic support (HR: 2.82 CI 1.21-6.55 p = 0.02). Furthermore, this severe VExUS grade offered a useful positive likelihood ratio (+LR: 6.37 CI 2.19-18.50) when detected at ICU admission, which outperformed central venous pressure measurements.
Conclusions: The combination of multiple POCUS markers may identify clinically significant venous congestion.
Keywords: Acute kidney injury; Cardiac surgery; Fluid balance; Point-Of-Care ultrasound; Venous congestion.
Conflict of interest statement
André Y. Denault is a Speaker for CAE Healthcare, Edwards and Masimo. The other authors have no conflict of interest to declare.
Figures
References
-
- van Diepen S, Katz Jason N, Albert Nancy M, Henry Timothy D, Jacobs Alice K, Kapur Navin K, Kilic A, Menon V, Ohman EM, Sweitzer Nancy K, Thiele H, Washam Jeffrey B, Cohen Mauricio G. Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation. 2017;136:e232–e268. doi: 10.1161/CIRCULATIONAHA.117.029532. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical