

Predicting Mortality in Children With Pediatric Acute Respiratory Distress Syndrome: A Pediatric Acute Respiratory Distress Syndrome Incidence and Epidemiology Study
- PMID: 32271186
- PMCID: PMC7237024
- DOI: 10.1097/CCM.0000000000004345
Predicting Mortality in Children With Pediatric Acute Respiratory Distress Syndrome: A Pediatric Acute Respiratory Distress Syndrome Incidence and Epidemiology Study
Abstract
Objectives: Pediatric acute respiratory distress syndrome is heterogeneous, with a paucity of risk stratification tools to assist with trial design. We aimed to develop and validate mortality prediction models for patients with pediatric acute respiratory distress syndrome.
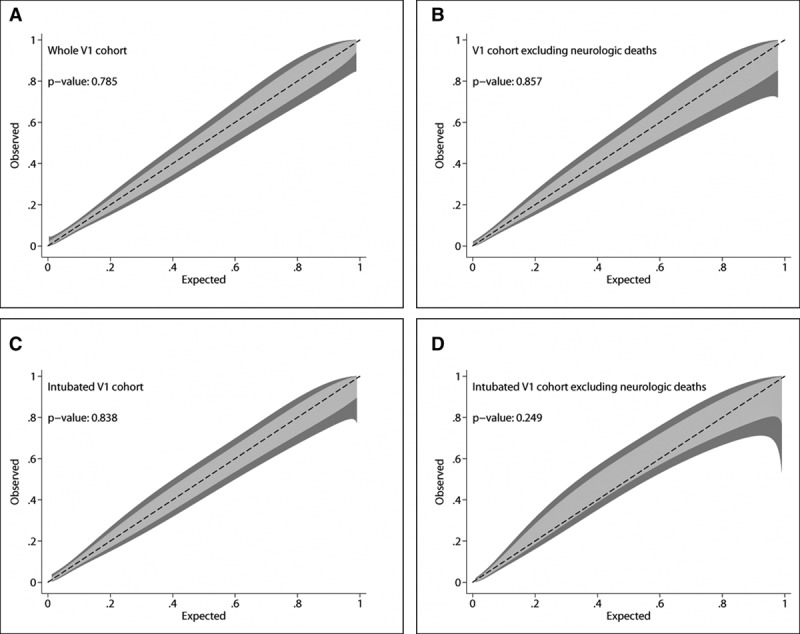
Design: Leveraging additional data collection from a preplanned ancillary study (Version 1) of the multinational Pediatric Acute Respiratory Distress syndrome Incidence and Epidemiology study, we identified predictors of mortality. Separate models were built for the entire Version 1 cohort, for the cohort excluding neurologic deaths, for intubated subjects, and for intubated subjects excluding neurologic deaths. Models were externally validated in a cohort of intubated pediatric acute respiratory distress syndrome patients from the Children's Hospital of Philadelphia.
Setting: The derivation cohort represented 100 centers worldwide; the validation cohort was from Children's Hospital of Philadelphia.
Patients: There were 624 and 640 subjects in the derivation and validation cohorts, respectively.
Interventions: None.
Measurements and main results: The model for the full cohort included immunocompromised status, Pediatric Logistic Organ Dysfunction 2 score, day 0 vasopressor-inotrope score and fluid balance, and PaO2/FIO2 6 hours after pediatric acute respiratory distress syndrome onset. This model had good discrimination (area under the receiver operating characteristic curve 0.82), calibration, and internal validation. Models excluding neurologic deaths, for intubated subjects, and for intubated subjects excluding neurologic deaths also demonstrated good discrimination (all area under the receiver operating characteristic curve ≥ 0.84) and calibration. In the validation cohort, models for intubated pediatric acute respiratory distress syndrome (including and excluding neurologic deaths) had excellent discrimination (both area under the receiver operating characteristic curve ≥ 0.85), but poor calibration. After revision, the model for all intubated subjects remained miscalibrated, whereas the model excluding neurologic deaths showed perfect calibration. Mortality models also stratified ventilator-free days at 28 days in both derivation and validation cohorts.
Conclusions: We describe predictive models for mortality in pediatric acute respiratory distress syndrome using readily available variables from day 0 of pediatric acute respiratory distress syndrome which outperform severity of illness scores and which demonstrate utility for composite outcomes such as ventilator-free days. Models can assist with risk stratification for clinical trials.
Conflict of interest statement
Dr. Yehya’s institution received funding from National Heart, Lung, and Blood Institute and Pfizer. Drs. Yehya, Harhay, Sapru, and Flori received support for article research from the National Institutes of Health (NIH). Dr. Klein received support from University of Southern California Clinical Translational Science Institute; CHU Sainte-Justine, University of Montreal, Canada; Réseau en Santé Respiratoire du Fonds de Recherche Quebec - Santé (FRQS); and Children’s Hospital Los Angeles, Department of Anesthesiology and Critical Care Medicine. Additional individual funding received from K23-HL136688 (to Dr. Yehya); R00-HL141678 (to Dr. Harhay); Fonds de recherche du Québec Santé (to Dr. Emeriaud); K12-HD047349 (to Dr. Haileselassie); Stanford Maternal Child Health Research Institute Early Career Award (to Dr. Haileselassie); UG3-HL141736 (to Dr. Kneyber); UL1-TR000457 (to Dr. Hsing); and Parker B. Francis Fellowship Program (to Dr. Maddux). Dr. Emeriaud’s institution received funding from FRQS, and he disclosed that he is the principal investigator of a feasibility study of a new ventilator which is financially supported by Maquet Critical Care. Dr. Flori received funding from Thermo Fisher Scientific (scientific advisory), Aerogen Pharma (scientific advisory), the Society of Critical Care Medicine (travel support), and the Michigan Thoracic Society (Board of Directors). Dr. Maddux’s institution received funding from Parker B. Francis Foundation (Fellowship award). Dr. Khemani’s institution received funding from Los Angeles Basin Clinical Translational Science Institute through the NIH; received support for article research from Southern California Clinical and Translational Science Institute. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Ashbaugh DG, Bigelow DB, Petty TL, et al. Acute respiratory distress in adults. Lancet 1967; 2:319–323 - PubMed
-
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994; 149:818–824 - PubMed
-
- Ranieri VM, Rubenfeld GD, Thompson BT, et al. ; ARDS Definition Task Force: Acute respiratory distress syndrome: The Berlin definition. JAMA 2012; 307:2526–2533 - PubMed
-
- Khemani RG, Smith LS, Zimmerman JJ, et al. ; Pediatric Acute Lung Injury Consensus Conference Group: Pediatric acute respiratory distress syndrome: Definition, incidence, and epidemiology: Proceedings from the Pediatric Acute Lung Injury Consensus Conference. Pediatr Crit Care Med 2015; 16:S23–S40 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
