

Assessment of the Feasibility and Safety of Durvalumab for Treatment of Solid Tumors in Patients With HIV-1 Infection: The Phase 2 DURVAST Study
- PMID: 32271353
- PMCID: PMC7146525
- DOI: 10.1001/jamaoncol.2020.0465
Assessment of the Feasibility and Safety of Durvalumab for Treatment of Solid Tumors in Patients With HIV-1 Infection: The Phase 2 DURVAST Study
Abstract
Importance: Therapies targeting the programmed cell death 1 (PD-1) receptor or its ligand (PD-L1), such as the humanized monoclonal antibody durvalumab, have shown durable clinical responses in several tumor types. However, concerns about the safety and feasibility of PD-1/PD-L1 blockade in HIV-1-infected individuals have led to the exclusion of these patients from clinical trials on cancer immunotherapies.
Objective: To evaluate the feasibility and safety of durvalumab treatment in patients with advanced cancer and virologically controlled HIV-1 infection.
Design, setting, and participants: The DURVAST study was a nonrandomized, open-label, phase 2 clinical trial in patients with any solid tumor type in which anti-PD-1 or anti-PD-L1 antibodies have approved indications or for which there are data of antitumoral activity with no other available curative therapy. All patients had basal undetectable plasma viremia while undergoing combination antiretroviral therapy.
Interventions: Treatment consisted of intravenous infusion of durvalumab (1500 mg every 4 weeks) until disease progression or unacceptable toxic effects.
Main outcomes and measures: Adverse events were graded with the use of the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.03. Tumor response was evaluated using the Response Evaluation Criteria in Solid Tumors version 1.1.
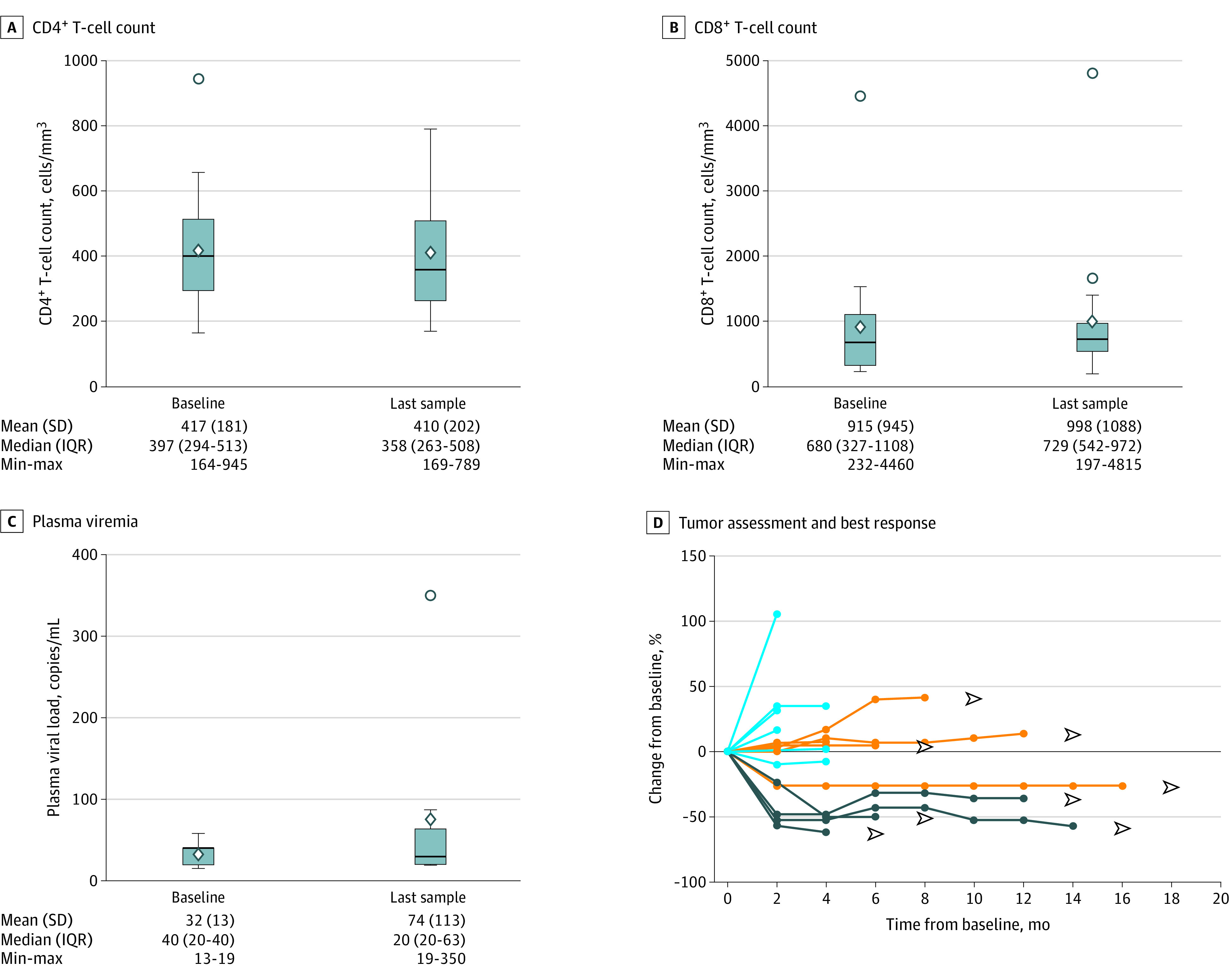
Results: A total of 20 HIV-1-infected patients with advanced cancer were enrolled; 16 (80%) were male, the median (range) age was 54 (30-73) years, and 12 (60%) had progressed with previous cancer treatment lines. A median (range) of 4 (1-16) cycles of durvalumab were administered. Drug-related adverse events were observed in 50% of patients, and all were grade 1 and 2 (mainly diarrhea, asthenia, and arthromyalgia). Four of 16 response-evaluable patients (25%) had a partial response. Five patients (31%) had stable disease, including 4 with durable stable disease (disease control rate of 50%). CD4+ and CD8+ T-cell counts and plasma HIV-1 viremia remained stable throughout the study.
Conclusions and relevance: Durvalumab treatment was feasible and safe in HIV-1-infected patients with cancer receiving combination antiretroviral therapy. HIV-1-infected patients on suppressive antiretroviral therapy with advanced cancer should have access to cancer immunotherapy treatments.
Trial registration: ClinicalTrials.gov Identifier: NCT03094286.
Conflict of interest statement
Figures
Comment in
-
Safety of Anti-PD-L1 Inhibition in HIV-1-Infected Patients With Cancer-Reply.JAMA Oncol. 2020 Nov 1;6(11):1810-1811. doi: 10.1001/jamaoncol.2020.3400. JAMA Oncol. 2020. PMID: 32910172 No abstract available.
-
Safety of Anti-PD-L1 Inhibition in HIV-1-Infected Patients With Cancer.JAMA Oncol. 2020 Nov 1;6(11):1810. doi: 10.1001/jamaoncol.2020.3389. JAMA Oncol. 2020. PMID: 32910177 No abstract available.
