

All-Cause Mortality and Serious Non-AIDS Events in Adults With Low-level Human Immunodeficiency Virus Viremia During Combination Antiretroviral Therapy: Results From a Swedish Nationwide Observational Study
- PMID: 32271361
- PMCID: PMC8204776
- DOI: 10.1093/cid/ciaa413
All-Cause Mortality and Serious Non-AIDS Events in Adults With Low-level Human Immunodeficiency Virus Viremia During Combination Antiretroviral Therapy: Results From a Swedish Nationwide Observational Study
Abstract
Background: The impact of low levels of human immunodeficiency virus (HIV) RNA (low-level viremia [LLV]) during combination antiretroviral therapy (cART) on clinical outcomes is unclear. We explored the associations between LLV and all-cause mortality, AIDS, and serious non-AIDS events (SNAEs).
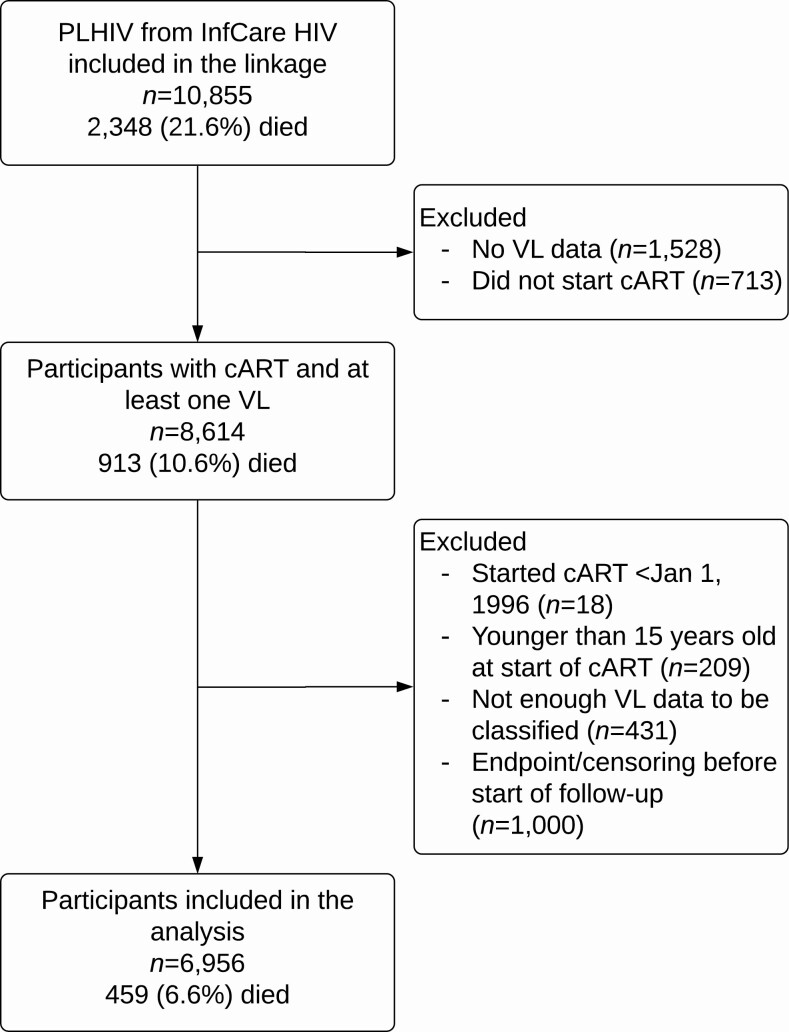
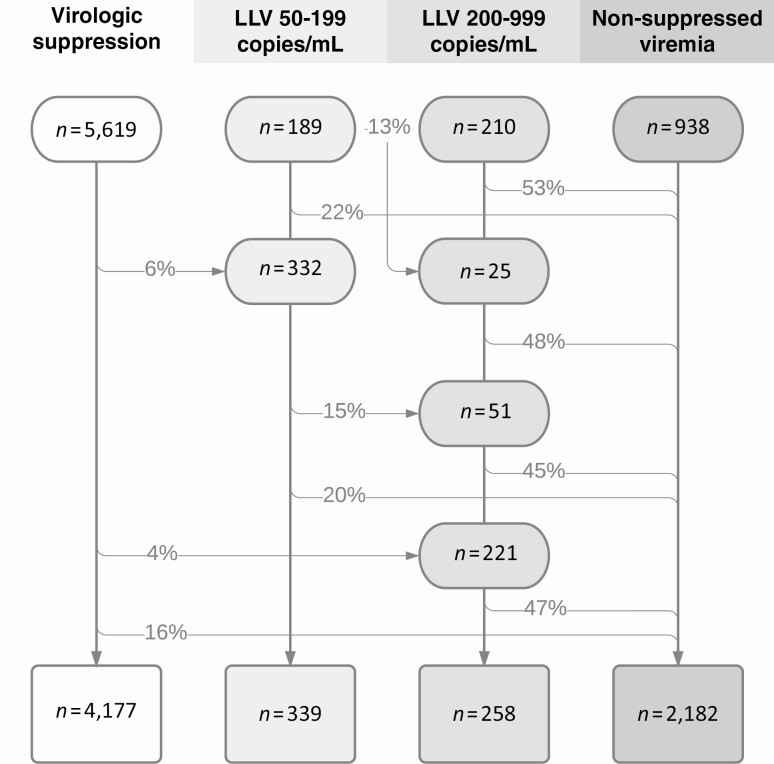
Methods: We grouped individuals starting cART 1996-2017 (identified from the Swedish InfCare HIV register) as virologic suppression (VS; <50 copies/mL), LLV (repeated viral load, 50-999 copies/mL), and nonsuppressed viremia (NSV; ≥1000 copies/mL). Separately, LLV was subdivided into 50-199 and 200-999 copies/mL (reflecting different definitions of virologic failure). Proportional-hazard models (including sex, age, pre-ART CD4 count and viral load, country of birth, injection drug use, treatment experience and interruptions, and an interaction term between viremia and time) were fitted for the study outcomes.
Results: A total of 6956 participants were followed for a median of 5.7 years. At the end of follow-up, 60% were categorized as VS, 9% as LLV, and 31% as NSV. Compared with VS, LLV was associated with increased mortality (adjusted hazard ratio [aHR], 2.2; 95% confidence interval [CI], 1.3-3.6). This association was also observed for LLV 50-199 copies/mL (aHR, 2.2; 95% CI, 1.3-3.8), but was not statistically significant for LLV 200-999 copies/mL (aHR, 2.1; 95% CI, .96-4.7). LLV 50-999 copies/mL was not linked to increased risk of AIDS or SNAEs, but in subanalysis, LLV 200-999 copies/mL was associated with SNAEs (aHR, 2.0; 95% CI, 1.2-3.6).
Conclusions: In this population-based cohort, LLV during cART was associated with adverse clinical outcomes.
Keywords: HIV; antiretroviral therapy; low-level viremia; mortality; serious non-AIDS events.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Croxford S, Kitching A, Desai S, et al. . Mortality and causes of death in people diagnosed with HIV in the era of highly active antiretroviral therapy compared with the general population: an analysis of a national observational cohort. Lancet Public Health 2017; 2:e35–46. - PubMed
-
- Smith CJ, Ryom L, Weber R, et al. . Trends in underlying causes of death in people with HIV from 1999 to 2011 (D:A:D): a multicohort collaboration. Lancet 2014; 384:241–8. - PubMed
-
- Helleberg M, Afzal S, Kronborg G, et al. . Mortality attributable to smoking among HIV-1-infected individuals: a nationwide, population-based cohort study. Clin Infect Dis 2013; 56:727–34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
