

Durvalumab With or Without Tremelimumab vs Standard Chemotherapy in First-line Treatment of Metastatic Non-Small Cell Lung Cancer: The MYSTIC Phase 3 Randomized Clinical Trial
- PMID: 32271377
- PMCID: PMC7146551
- DOI: 10.1001/jamaoncol.2020.0237
Durvalumab With or Without Tremelimumab vs Standard Chemotherapy in First-line Treatment of Metastatic Non-Small Cell Lung Cancer: The MYSTIC Phase 3 Randomized Clinical Trial
Erratum in
-
Incorrect Supplement Version.JAMA Oncol. 2020 Nov 1;6(11):1815. doi: 10.1001/jamaoncol.2020.5538. JAMA Oncol. 2020. PMID: 33001136 Free PMC article. No abstract available.
Abstract
Importance: Checkpoint inhibitors targeting programmed cell death 1 or its ligand (PD-L1) as monotherapies or in combination with anti-cytotoxic T-lymphocyte-associated antigen 4 have shown clinical activity in patients with metastatic non-small cell lung cancer.
Objective: To compare durvalumab, with or without tremelimumab, with chemotherapy as a first-line treatment for patients with metastatic non-small cell lung cancer.
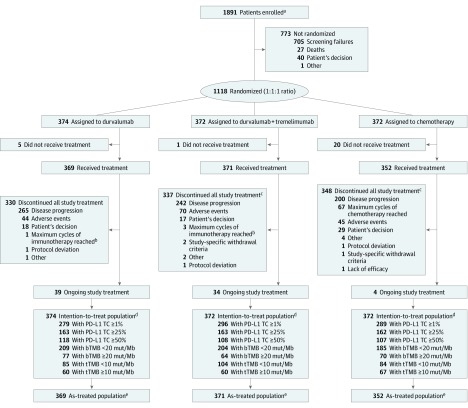
Design, setting, and participants: This open-label, phase 3 randomized clinical trial (MYSTIC) was conducted at 203 cancer treatment centers in 17 countries. Patients with treatment-naive, metastatic non-small cell lung cancer who had no sensitizing EGFR or ALK genetic alterations were randomized to receive treatment with durvalumab, durvalumab plus tremelimumab, or chemotherapy. Data were collected from July 21, 2015, to October 30, 2018.
Interventions: Patients were randomized (1:1:1) to receive treatment with durvalumab (20 mg/kg every 4 weeks), durvalumab (20 mg/kg every 4 weeks) plus tremelimumab (1 mg/kg every 4 weeks, up to 4 doses), or platinum-based doublet chemotherapy.
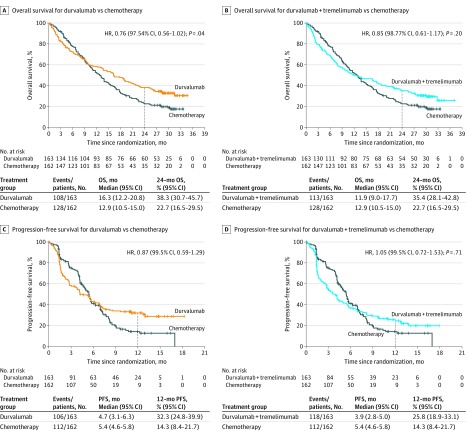
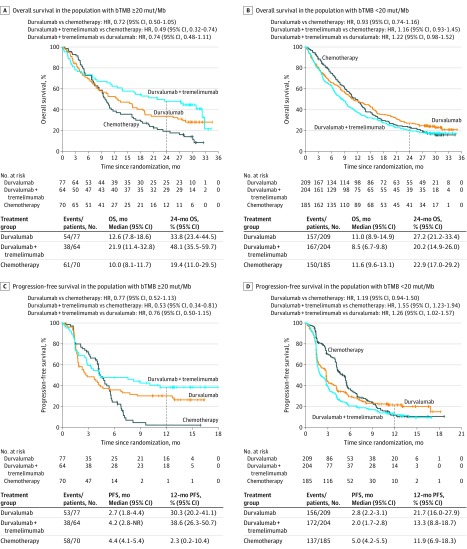
Main outcomes and measures: The primary end points, assessed in patients with ≥25% of tumor cells expressing PD-L1, were overall survival (OS) for durvalumab vs chemotherapy, and OS and progression-free survival (PFS) for durvalumab plus tremelimumab vs chemotherapy. Analysis of blood tumor mutational burden (bTMB) was exploratory.
Results: Between July 21, 2015, and June 8, 2016, 1118 patients were randomized. Baseline demographic and disease characteristics were balanced between treatment groups. Among 488 patients with ≥25% of tumor cells expressing PD-L1, median OS was 16.3 months (95% CI, 12.2-20.8) with durvalumab vs 12.9 months (95% CI, 10.5-15.0) with chemotherapy (hazard ratio [HR], 0.76; 97.54% CI, 0.56-1.02; P = .04 [nonsignificant]). Median OS was 11.9 months (95% CI, 9.0-17.7) with durvalumab plus tremelimumab (HR vs chemotherapy, 0.85; 98.77% CI, 0.61-1.17; P = .20). Median PFS was 3.9 months (95% CI, 2.8-5.0) with durvalumab plus tremelimumab vs 5.4 months (95% CI, 4.6-5.8) with chemotherapy (HR, 1.05; 99.5% CI, 0.72-1.53; P = .71). Among 809 patients with evaluable bTMB, those with a bTMB ≥20 mutations per megabase showed improved OS for durvalumab plus tremelimumab vs chemotherapy (median OS, 21.9 months [95% CI, 11.4-32.8] vs 10.0 months [95% CI, 8.1-11.7]; HR, 0.49; 95% CI, 0.32-0.74). Treatment-related adverse events of grade 3 or higher occurred in 55 (14.9%) of 369 patients who received treatment with durvalumab, 85 (22.9%) of 371 patients who received treatment with durvalumab plus tremelimumab, and 119 (33.8%) of 352 patients who received treatment with chemotherapy. These adverse events led to death in 2 (0.5%), 6 (1.6%), and 3 (0.9%) patients, respectively.
Conclusions and relevance: The phase 3 MYSTIC study did not meet its primary end points of improved OS with durvalumab vs chemotherapy or improved OS or PFS with durvalumab plus tremelimumab vs chemotherapy in patients with ≥25% of tumor cells expressing PD-L1. Exploratory analyses identified a bTMB threshold of ≥20 mutations per megabase for optimal OS benefit with durvalumab plus tremelimumab.
Trial registration: ClinicalT rials.gov Identifier: NCT02453282.
Conflict of interest statement
Figures
Comment in
-
The Mystic Role of Tumor Mutational Burden in Selecting Patients With Lung Cancer for First-Line Immunotherapy.JAMA Oncol. 2020 May 1;6(5):674-675. doi: 10.1001/jamaoncol.2020.0264. JAMA Oncol. 2020. PMID: 32271363 No abstract available.
References
-
- Mok TSK, Wu YL, Kudaba I, et al. ; KEYNOTE-042 Investigators . Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819-1830. doi: 10.1016/S0140-6736(18)32409-7 - DOI - PubMed
-
- West H, McCleod M, Hussein M, et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019;20(7):924-937. doi: 10.1016/S1470-2045(19)30167-6 - DOI - PubMed
-
- Papadimitrakopoulou VA, Cobo M, Bordoni R, et al. IMpower132: PFS and safety results with 1L atezolizumab + carboplatin/cisplatin + pemetrexed in stage IV non-squamous NSCLC [abstract OA05.07]. J Thorac Oncol. 2018;13(10)(suppl):S332-S333. doi: 10.1016/j.jtho.2018.08.262 - DOI
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
