

The interplay between innate and adaptive immunity in cancer shapes the productivity of cancer immunosurveillance
- PMID: 32272502
- PMCID: PMC7377219
- DOI: 10.1002/JLB.3MIR0320-475R
The interplay between innate and adaptive immunity in cancer shapes the productivity of cancer immunosurveillance
Abstract
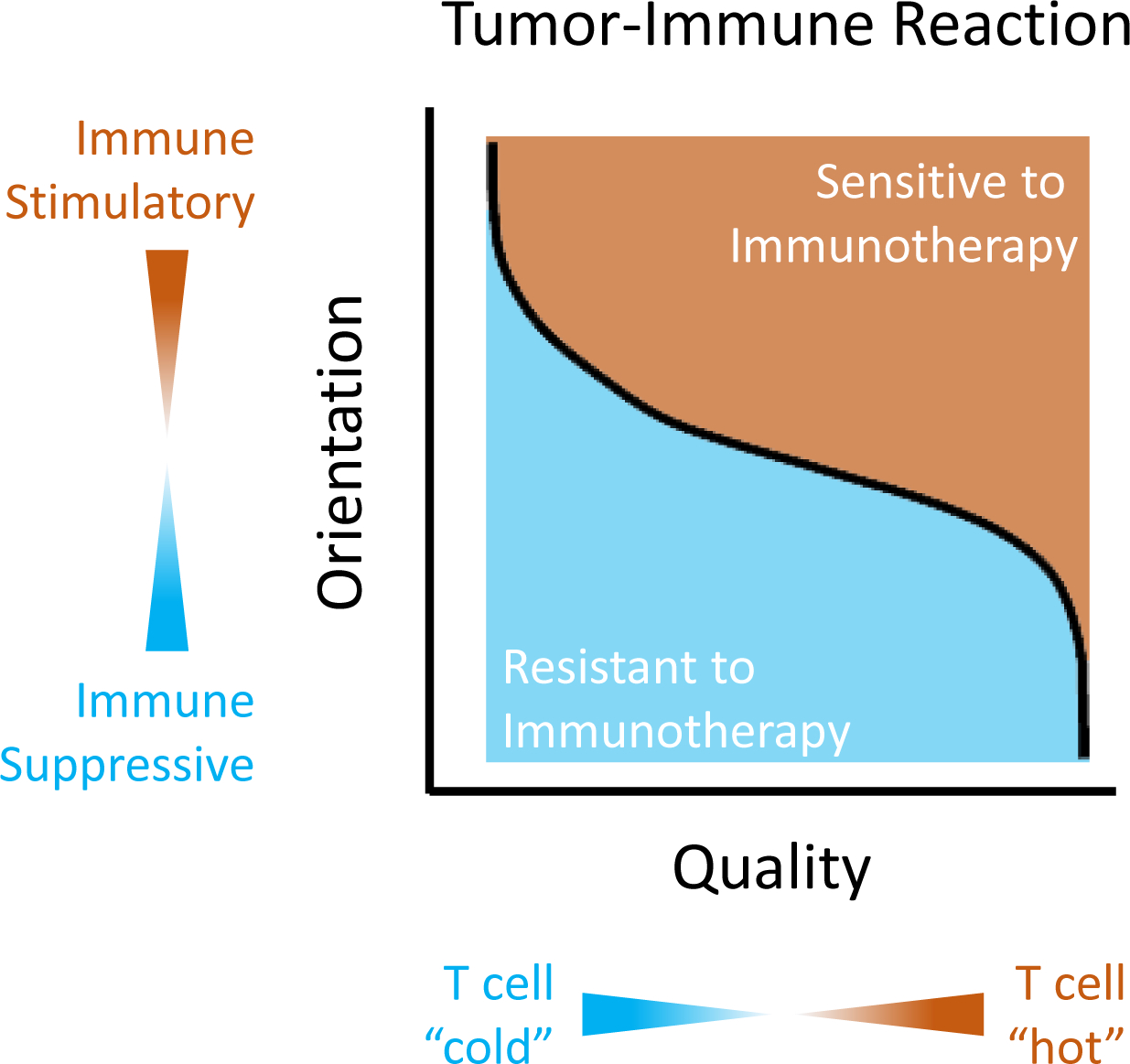
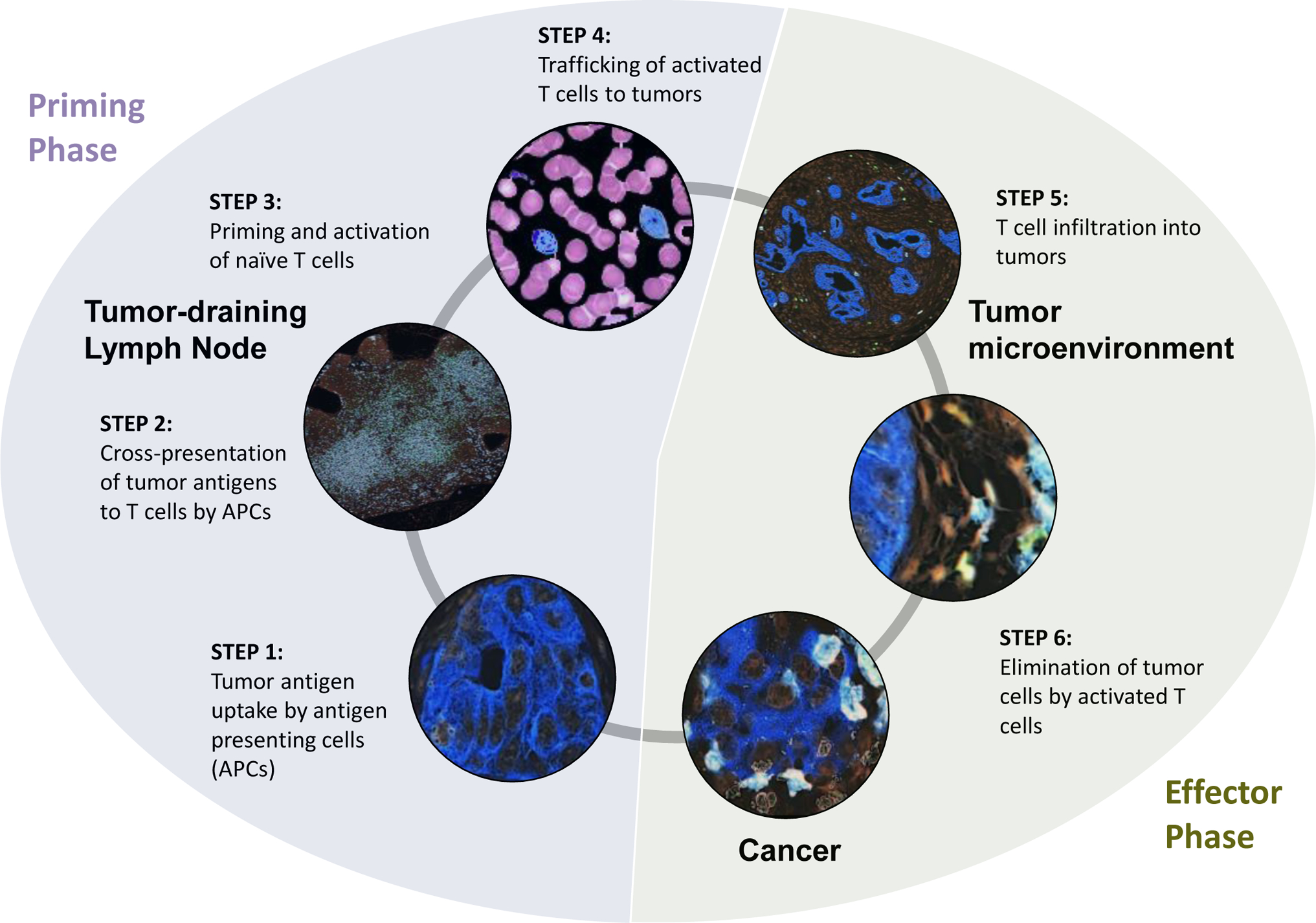
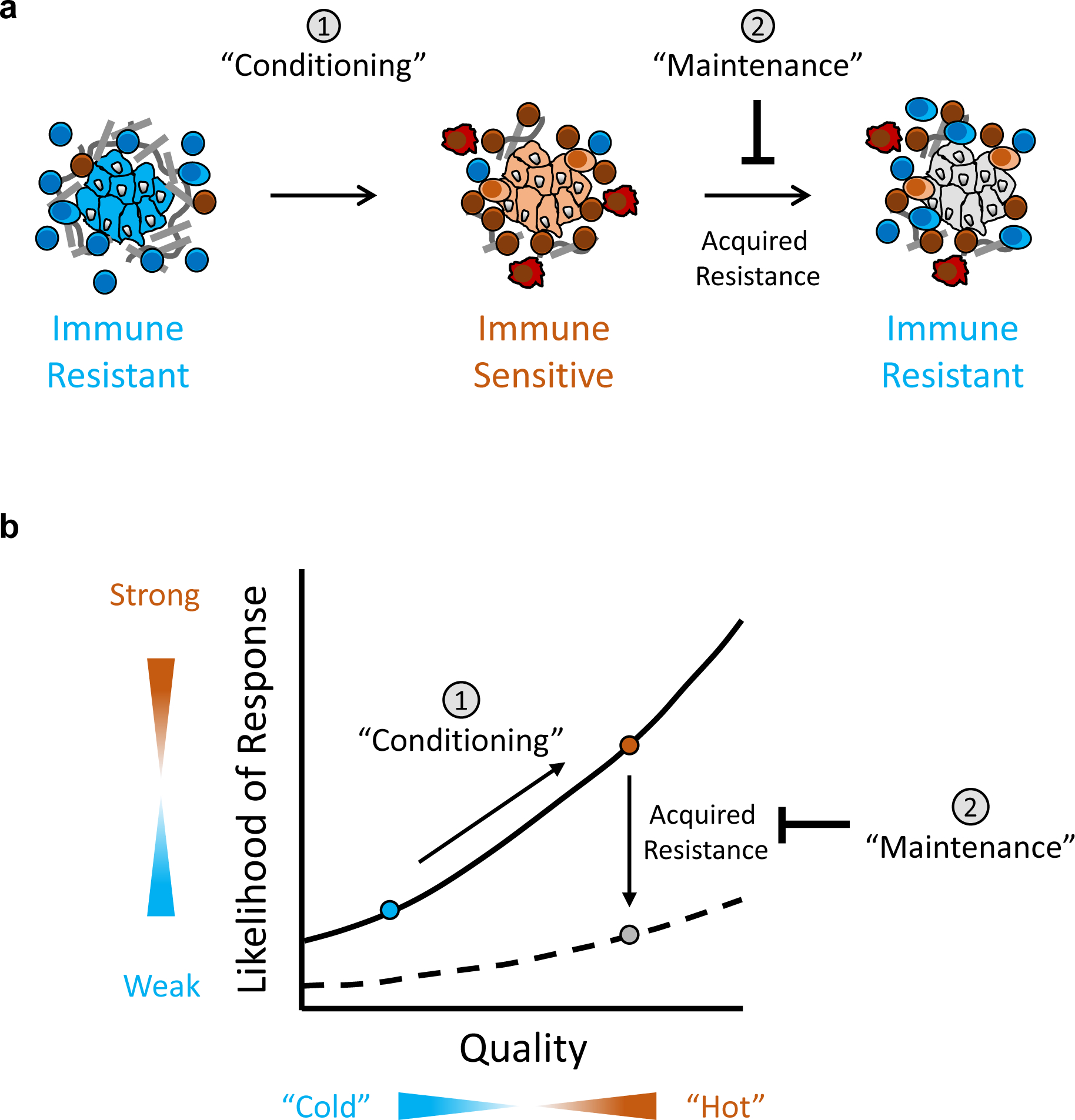
The immune system is a vital determinant of cancer and shapes its trajectory. Notably, the immune reaction to cancer harbors dual potential for suppressing or promoting cancer development and progression. This polarity of the immune response is determined, in part, by the character of the interplay between innate and adaptive immunity. On the one hand, the innate immune compartment is a necessary proponent of cancer immunity by supporting an immunostimulatory state that enables T cell immunosurveillance. However, in the setting of cancer, innate immune cells are commonly polarized with immune-suppressive properties and as a result, orchestrate a tolerogenic niche that interferes with the cytotoxic potential of tumor antigen-specific T cells. Here, we discuss the role of innate immunity as a positive and negative regulator of adaptive immunosurveillance; moreover, we highlight how tumor cells may skew leukocytes toward an immunosuppressive state and, as such, subvert the phenotypic plasticity of the immune compartment to advance disease progression. These observations establish the precedent for novel therapeutic strategies that aim to restore the tumor microenvironment to an immunoreactive state and, in doing so, condition and maintain the immunogenicity of tumors to yield deep and durable responses to immunotherapy.
Keywords: T cells; cancer; conditioning therapy; immune evasion; immunotherapy; maintenance therapy; myeloid cells.
©2020 Society for Leukocyte Biology.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest: G.L.B. is a consultant/advisory board member for Seattle Genetics, Aduro Biotech, AstraZeneca, Bristol-Myers Squibb, Incyte, Genmab, Takeda, Merck, and BiolineRx; reports receiving commercial research grants from Incyte, Bristol-Myers Squibb, Verastem, Halozyme, Biothera, Newlink, Novartis, Arcus, and Janssen; and is an inventor of intellectual property and recipient of royalties from Novartis and Advaxis, Inc. No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- Hanahan D, Weinberg RA. Hallmarks of Cancer: The Next Generation. Cell. 2011;144:646–674. - PubMed
-
- Pitt JM, Vétizou M, Daillère R, et al. Resistance Mechanisms to Immune-Checkpoint Blockade in Cancer: Tumor-Intrinsic and -Extrinsic Factors. Immunity. 2016;44:1255–1269. - PubMed
-
- Dunn GP, Old LJ, Schreiber RD. The Immunobiology of Cancer Immunosurveillance and Immunoediting. Immunity. 2004;21:137–148. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
