

Predictive factors influencing pregnancy rate in frozen embryo transfer
- PMID: 32273825
- PMCID: PMC7138944
- DOI: 10.1002/rmb2.12322
Predictive factors influencing pregnancy rate in frozen embryo transfer
Abstract
Purpose: To evaluate the outcomes of embryo transfer (ET) and to identify the parameters influencing pregnancy outcomes.
Methods: This study included 938 ET cycles involving single frozen and thawed good-quality blastocyst (Gardner grade ≥3BB) between August 2017 and January 2018. The significance of several parameters including endometrial thickness, position of the transferred air bubble, self-evaluation score by physicians, and uterus direction at ET as predictors of clinical pregnancy was evaluated using univariate and multivariate analyses.
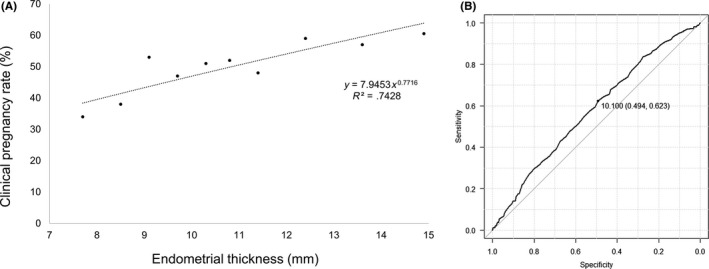
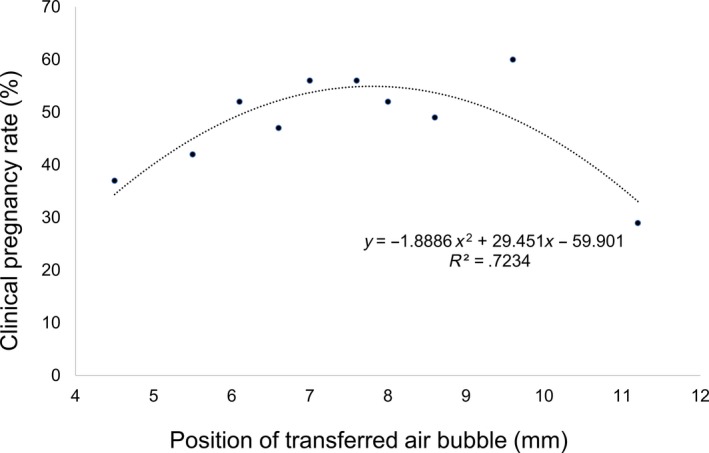
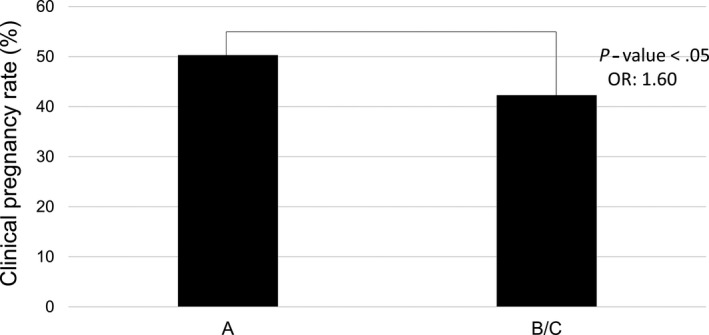
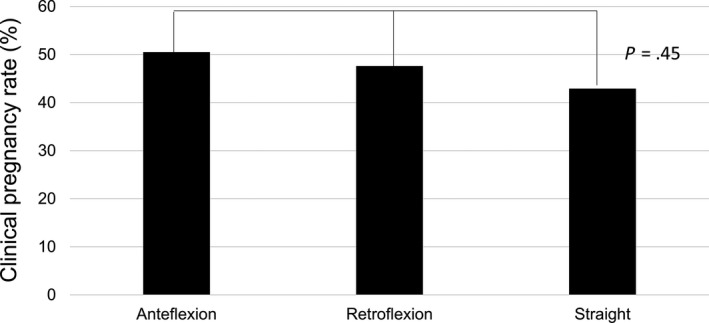
Results: Among 938 ET cycles, 462 (49.3%) resulted in a clinical pregnancy. Endometrial thickness was positively associated with clinical pregnancy in a linear trend. Between the variable position of the transferred air bubble and clinical pregnancy rate showed a curvilinear relationship. Clinical pregnancy rate was higher in cases with good self-evaluation score, whereas there was no difference between groups with different uterus directions. Univariate analysis of predictive parameters identified endometrial thickness, self-evaluation score by physicians, and position of air bubbles as significant predictors of clinical pregnancy, of which endometrial thickness and position of air bubbles appeared to be independently related to clinical pregnancy.
Conclusion: Endometrial thickness and the position of transferred air bubbles influenced clinical pregnancy in ET cycles.
Keywords: assisted reproductive technique; clinical pregnancy rate; endometrial thickness; frozen‐thawed embryo transfer; predictive factors.
© 2020 The Authors. Reproductive Medicine and Biology published by John Wiley & Sons Australia, Ltd on behalf of Japan Society for Reproductive Medicine.
Conflict of interest statement
Conflict of interest: Nao Hayashi, Noritoshi Enatsu, Toshiro Iwasaki, Junko Otsuki, Yukiko Matsumoto, Shoji Kokeguchi, Masahide Shiotani declare that they have no conflict of interest. Human rights statement and informed consent: All patients were well informed, and written informed consent was obtained prior to the treatment period. The treatment investigated in this study has already been discussed in other studies that have shown positive outcomes. Animal studies: This article contains no studies with animal subjects performed by any of the authors. Approval by Ethics Committee: This study was approved by Ethical Committee of Hanabusa Women's Clinic consists of members chosen by our institute and third party medical institute (approval number; 2019‐08).
Figures
References
-
- Roseboom T, Vermeiden J, Schoute E, Lens J, Schats R. The probability of pregnancy after embryo transfer is affected by the age of the patient, cause of infertility, number of embryos transferred and the average morphology score, as revealed by multiple logistic regression analysis. Hum Reprod. 1995;10(11):3035‐3041. - PubMed
-
- Strandell A, Bergh C, Lundin K. Selection of patients suitable for one‐embryo transfer may reduce the rate of multiple births by half without impairment of overall birth rates. Hum Reprod. 2000;15(12):2520‐2525. - PubMed
-
- El‐Toukhy T, Coomarasamy A, Khairy M, et al. The relationship between endometrial thickness and outcome of medicated frozen embryo replacement cycles. Fertil Steril. 2008;89(4):832‐839. - PubMed
-
- Kojima K, Nomiyama M, Kumamoto T, Matsumoto Y, Iwasaka T. Transvaginal ultrasound‐guided embryo transfer improves pregnancy and implantation rates after IVF. Hum Reprod. 2001;16(12):2578‐2582. - PubMed
LinkOut - more resources
Full Text Sources