

Pulmonary veins variations with potential impact in thoracic surgery: a computed-tomography-based atlas
- PMID: 32274104
- PMCID: PMC7139082
- DOI: 10.21037/jtd.2020.01.34
Pulmonary veins variations with potential impact in thoracic surgery: a computed-tomography-based atlas
Abstract
Background: Pulmonary veins (PVs) are important during segmentectomy. Many case reports prove that they may be the source of bleeding during surgery, especially when anatomical variants are present. We decided to describe venous variations and prepare a computed tomography based atlas of our observations.
Methods: The study was conducted using 135 chest computed tomography studies with intra venous iodine contrast injection. The study population contained 86 females and 49 males, mean age was 60. Thirteen people had atrial fibrillation. Images were analysed using radiological workstation.
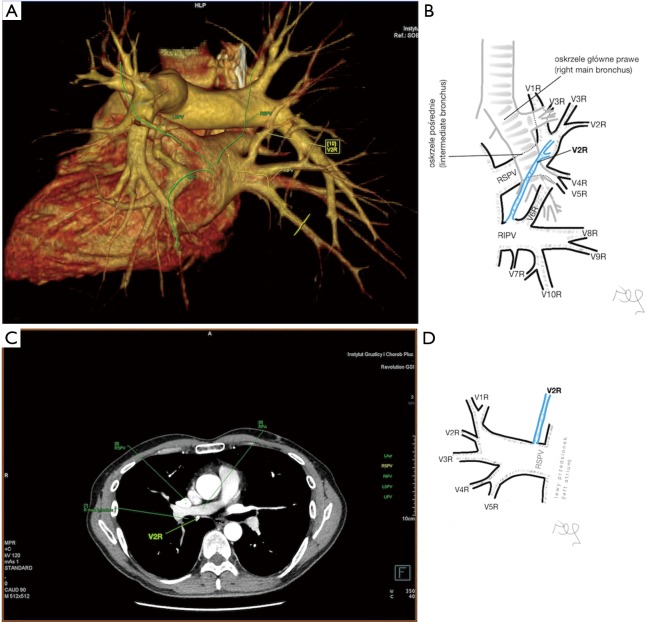
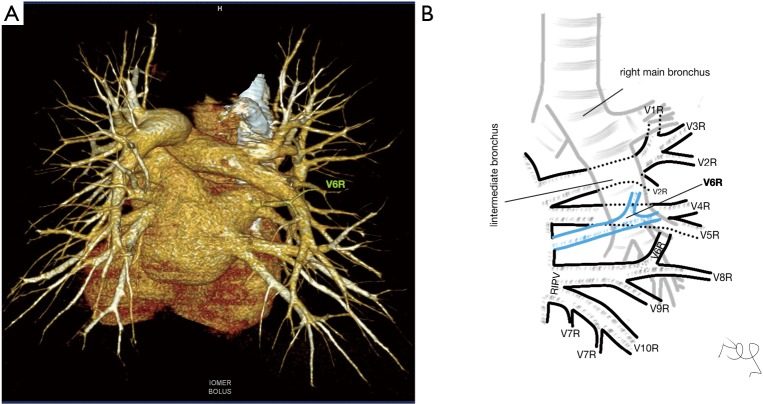
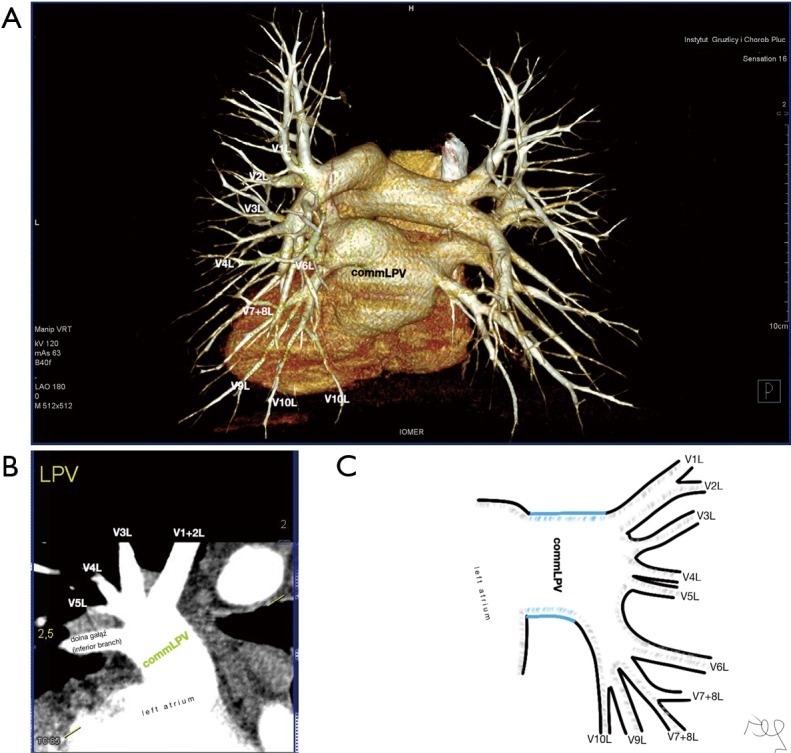
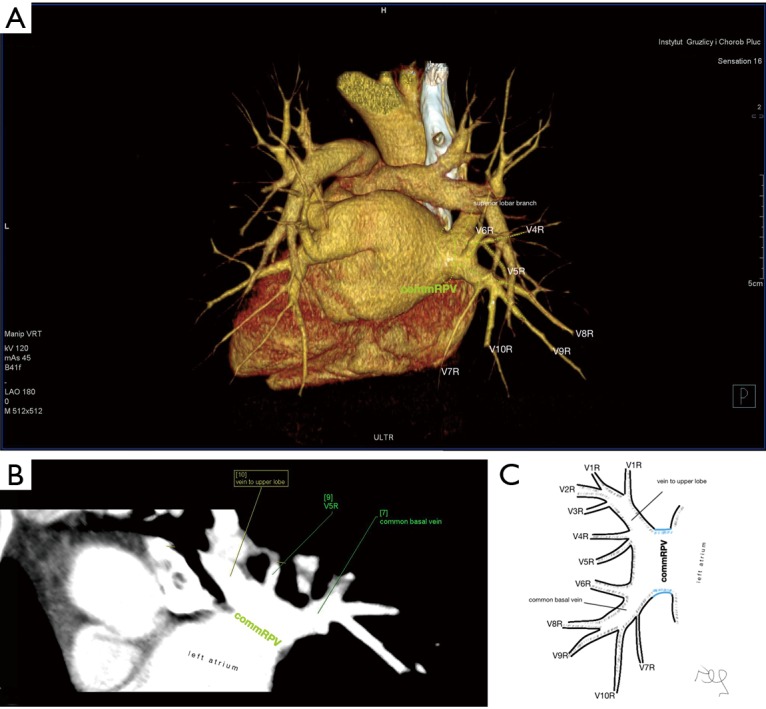
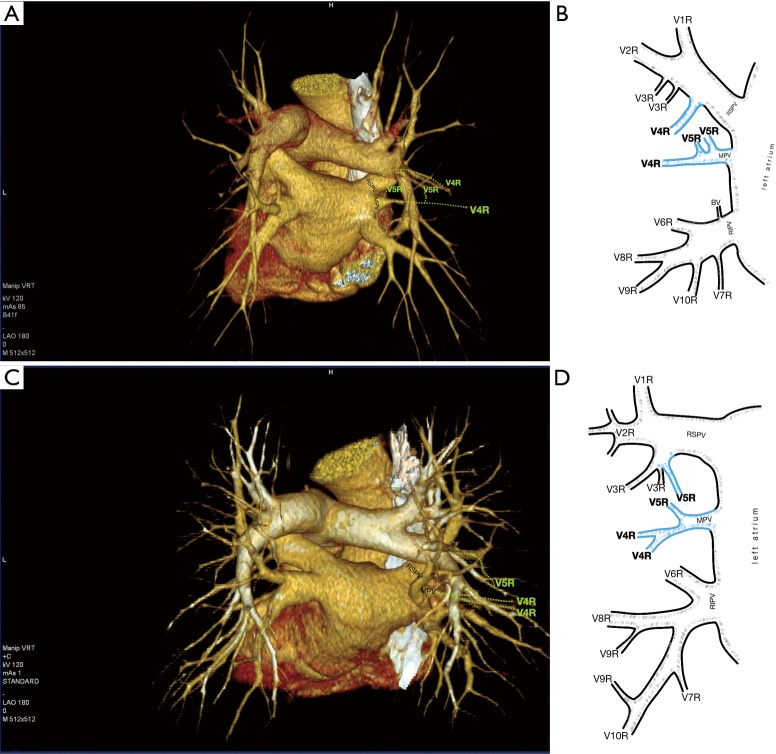
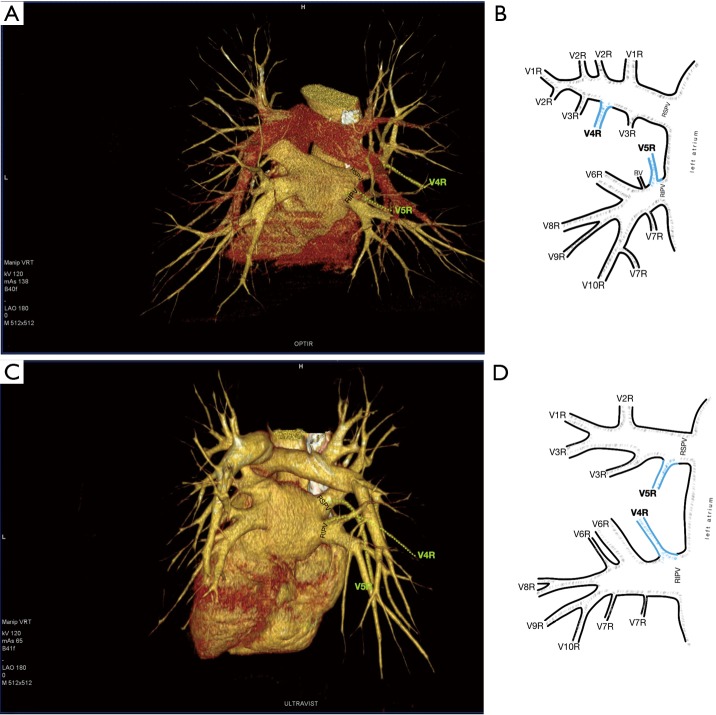
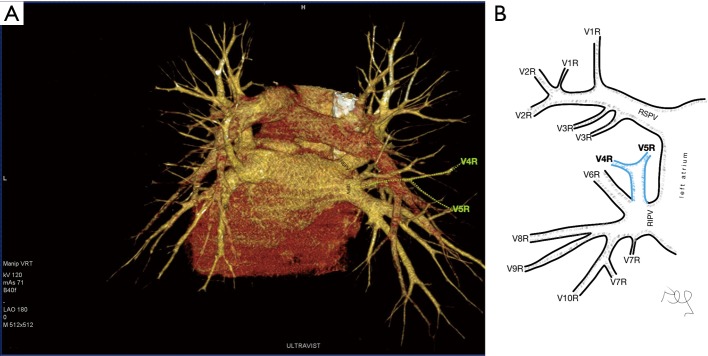
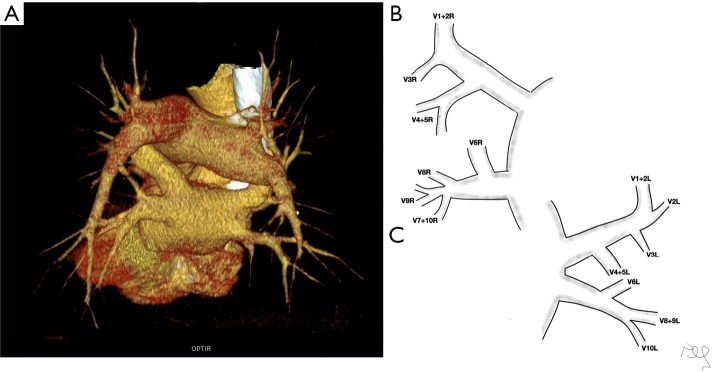
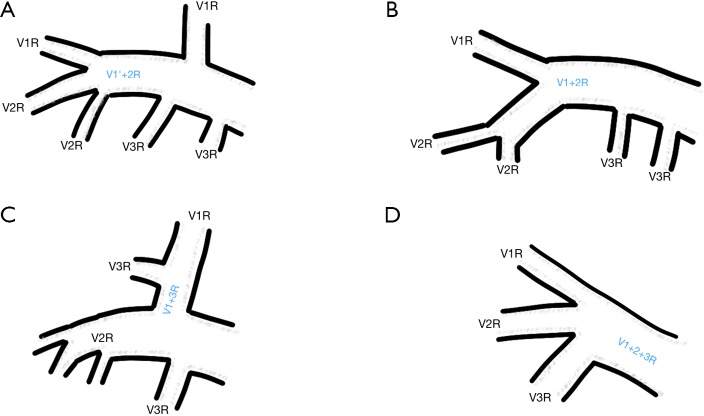
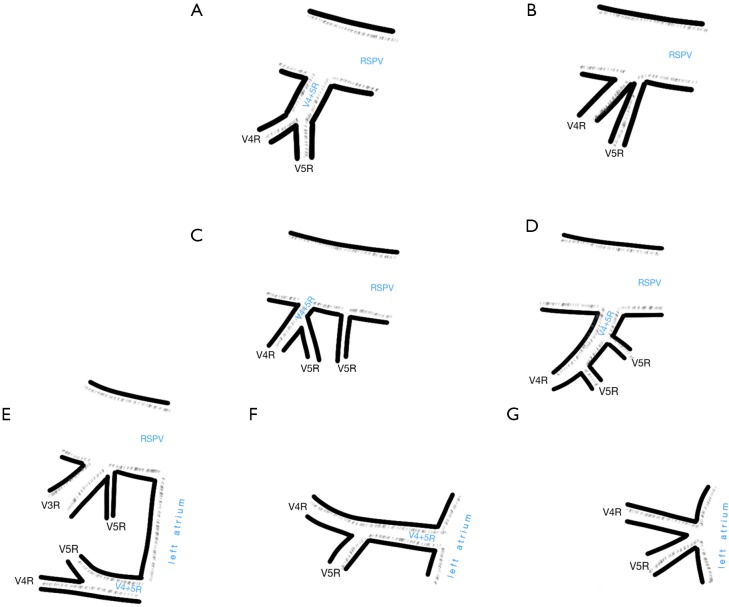
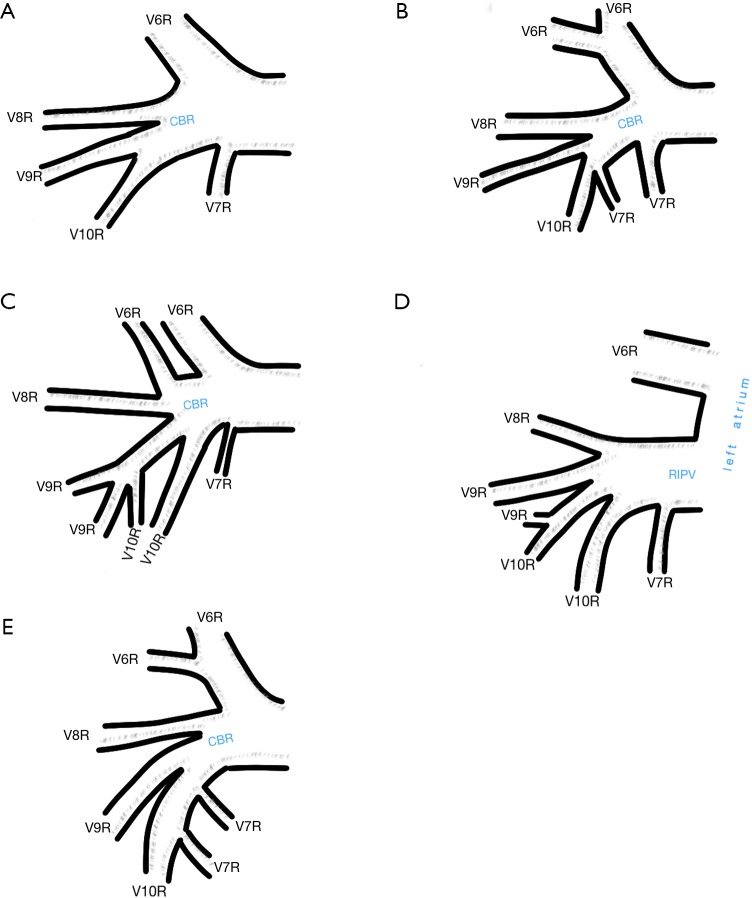
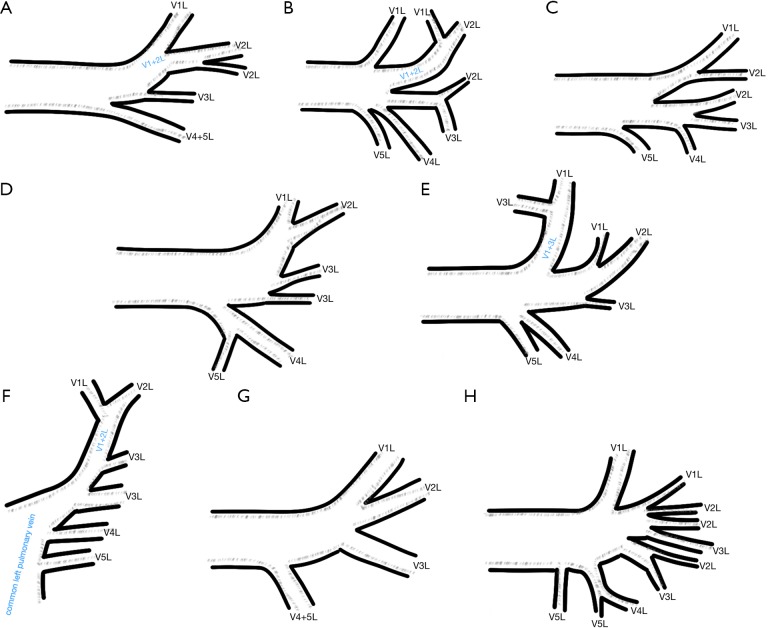
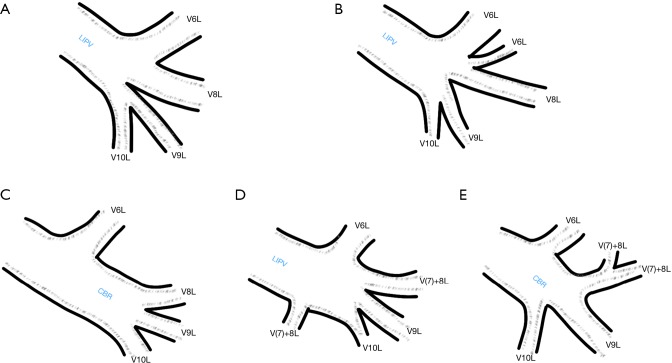
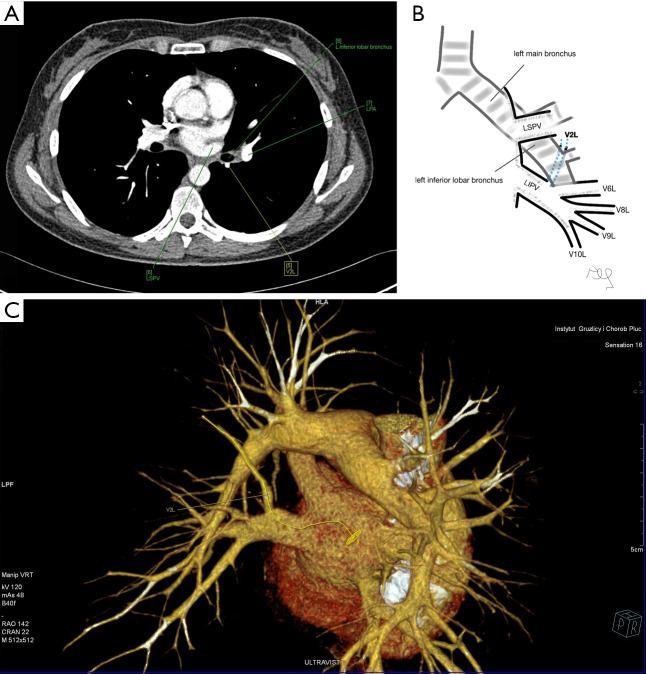
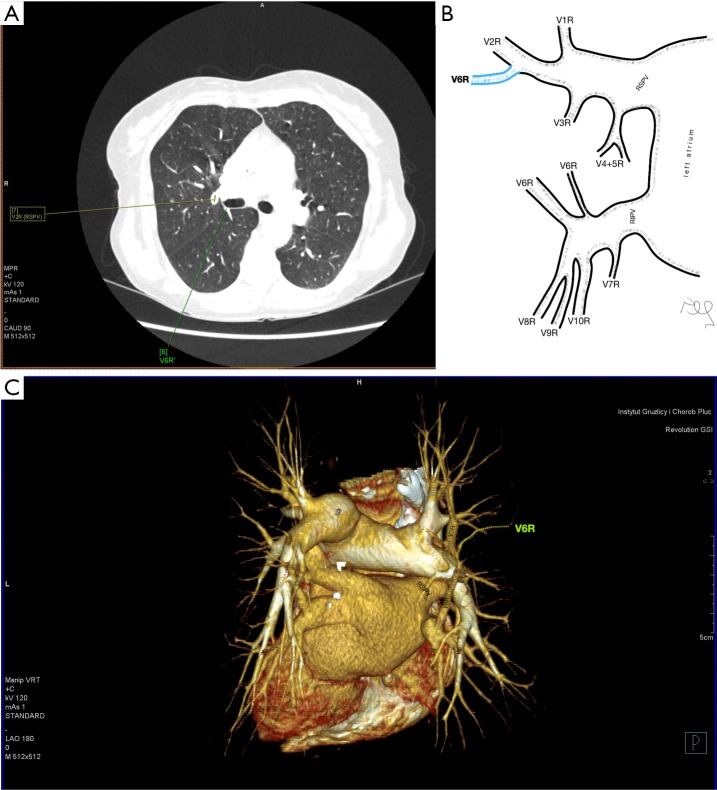
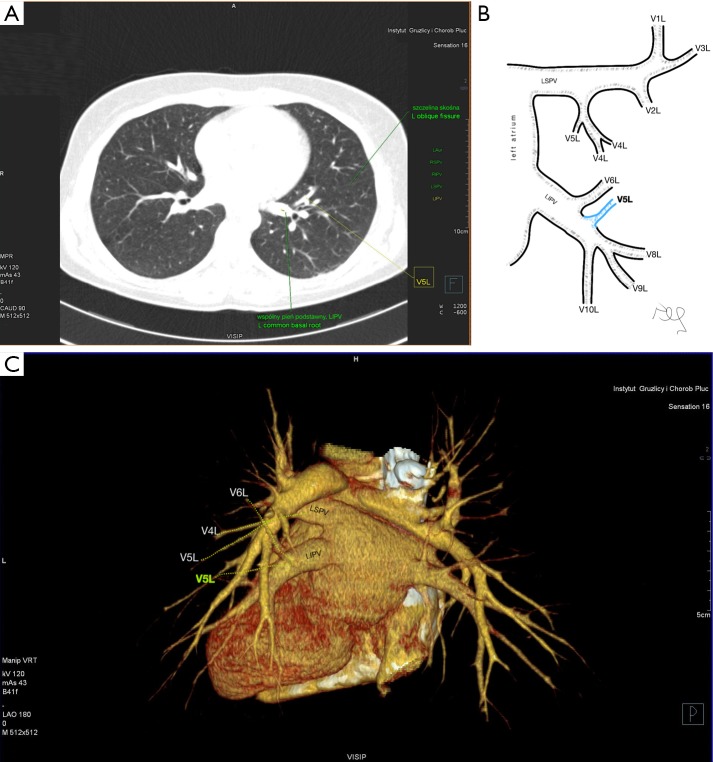
Results: The variations were divided into three categories: atypical topography of the PV, atypical venous outflow to the left atrium (LA), atypical venous vascularization of the lung bronchopulmonary segment. Retrobronchial course of the vein of the posterior segment of the right upper lobe was observed in 8.15%. The most common variant of atrial venous outflow was the direct outflow of the middle lobe vein, observed in 25.19% of cases and the long common trunk of left PVs in 11.11%. The split drainage from the middle lobe into the right superior pulmonary vein (RSPV) and the right inferior pulmonary vein (RIPV) was observed in 9.63% as the full drainage into the RIPV in 2.96%.
Conclusions: Long common trunk of left PVs and numerous variants of venous vascularisation of the middle lobe are the variations that may pose potential problems during thoracic surgeries. The frequency is high enough to justify the routine assessment of pulmonary vessels with computed tomography before surgery.
Keywords: Pulmonary veins (PVs); anatomy; computed tomography (CT); vascular complications.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
-
- Pearson FG, Cooper JD, Deslauriers J, et al. editors. Troracic Surgery. Second Edition. Philadelphia, Pensylvania: Churchill Livingstone, 2002:981-90.
LinkOut - more resources
Full Text Sources
Research Materials