

PaO2 greater than 300 mmHg promotes an inflammatory response during extracorporeal circulation in a rat extracorporeal membrane oxygenation model
- PMID: 32274141
- PMCID: PMC7139026
- DOI: 10.21037/jtd.2019.12.113
PaO2 greater than 300 mmHg promotes an inflammatory response during extracorporeal circulation in a rat extracorporeal membrane oxygenation model
Abstract
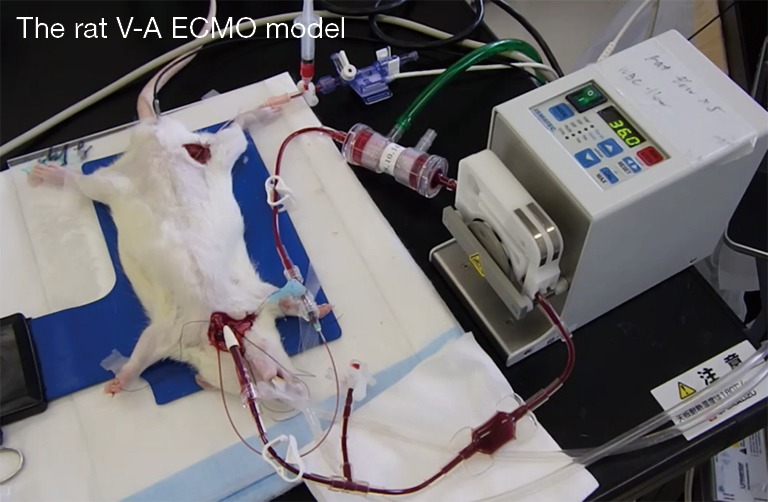
Background: Extracorporeal membrane oxygenation (ECMO) is being increasingly used for mechanical support of respiratory and cardio-circulatory failure. An excessive systemic inflammatory response is observed during sepsis and after cardiopulmonary bypass (CPB) with similar clinical features. We hypothesized that hyperoxia condition encourages the systemic inflammatory response and organ disorder during ECMO. To prove this hypothesis correct, we investigated the systemic inflammatory responses at normal and high levels of arterial oxygen pressure (PaO2) in the rat ECMO model.
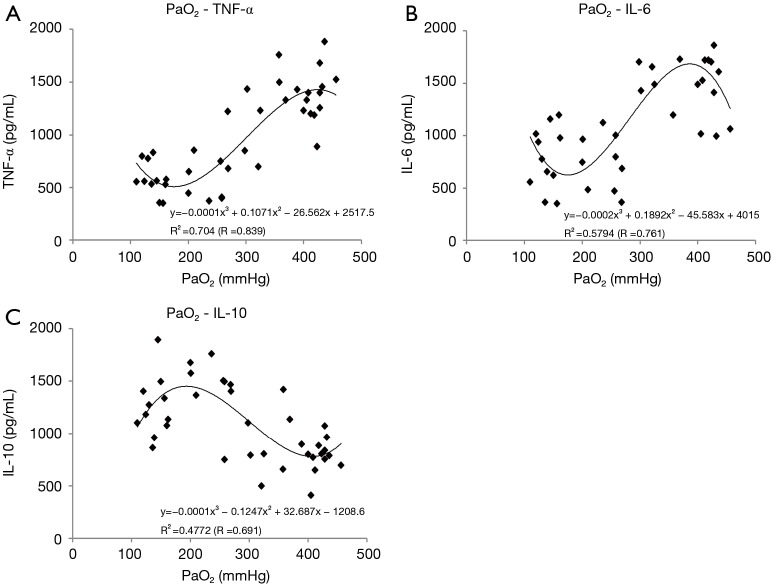
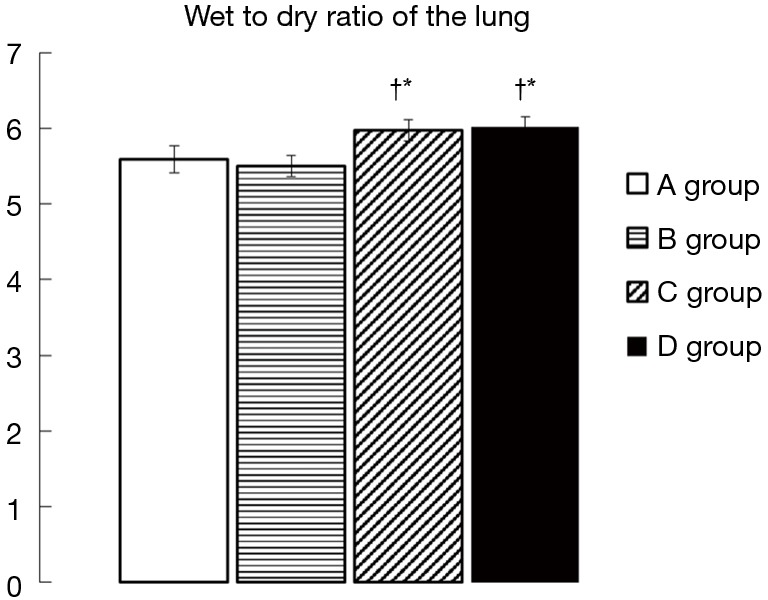
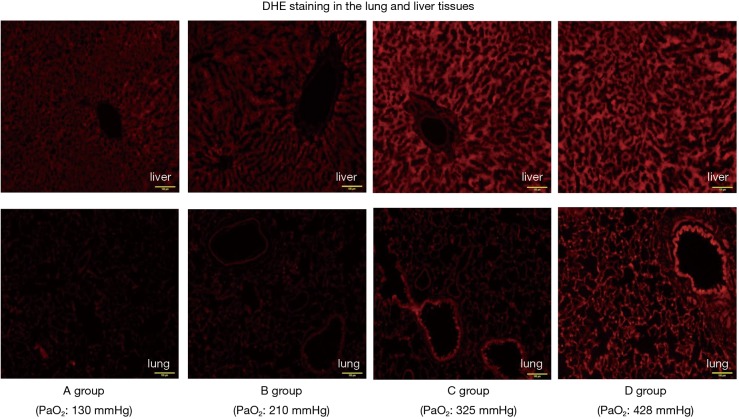
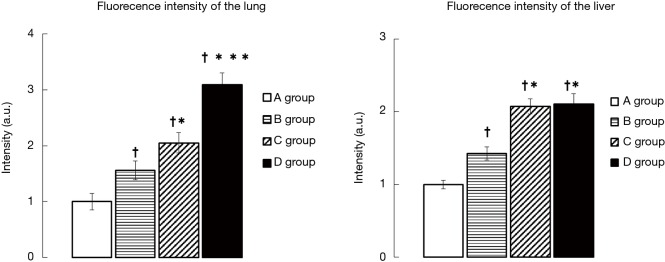
Methods: Rats were randomly assigned to one of the following groups depending on the value of PaO2 during ECMO: A group (n=11, PaO2 100-199 mmHg), B group (n=10, PaO2 200-299 mmHg), C group (n=8, PaO2 300-399 mmHg), and D group (n=11, PaO2 >400 mmHg). Serum cytokine levels [tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and interleukin-10 (IL-10)] were measured before, 60, and 120 min after the initiation of ECMO. The wet-to-dry weight (W/D) ratio of the left lung was also measured, and dihydroethidium (DHE) staining, reflecting superoxide generation, of lung and liver tissues was performed 120 min after ECMO initiation.
Results: In the C and D groups, the pro-inflammatory cytokines (TNF-α and IL-6) significantly increased during ECMO compared with the other groups. On the other hand, the increase in anti-inflammatory cytokines (IL-10) was more suppressed in the C and D groups than in the other groups. The W/D ratio increased significantly more in the C and D groups than in the other groups. In addition, DHE fluorescence had a tendency to increase as the PaO2 rose.
Conclusions: These data demonstrate that it is better to avoid administration of too much oxygen during ECMO to attenuate lung injury linked to generation of superoxide and the systemic inflammatory response.
Keywords: Extracorporeal circulation (ECC); cytokine; extracorporeal membrane oxygenation model (ECMO model); hyperoxia; superoxide; systemic inflammation.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form and declare: The authors have no conflicts of interest to declare.
Figures

References
LinkOut - more resources
Full Text Sources