Exercise MRI highlights heterogeneity in cardiovascular mechanics among patients with Fontan circulation: proposed protocol for routine evaluation
- PMID: 32274201
- PMCID: PMC7139092
- DOI: 10.21037/jtd.2019.09.59
Exercise MRI highlights heterogeneity in cardiovascular mechanics among patients with Fontan circulation: proposed protocol for routine evaluation
Abstract
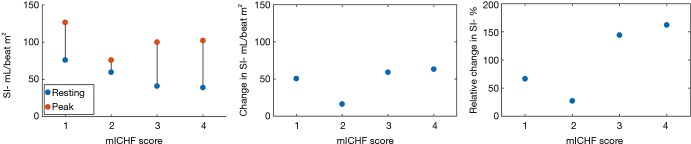
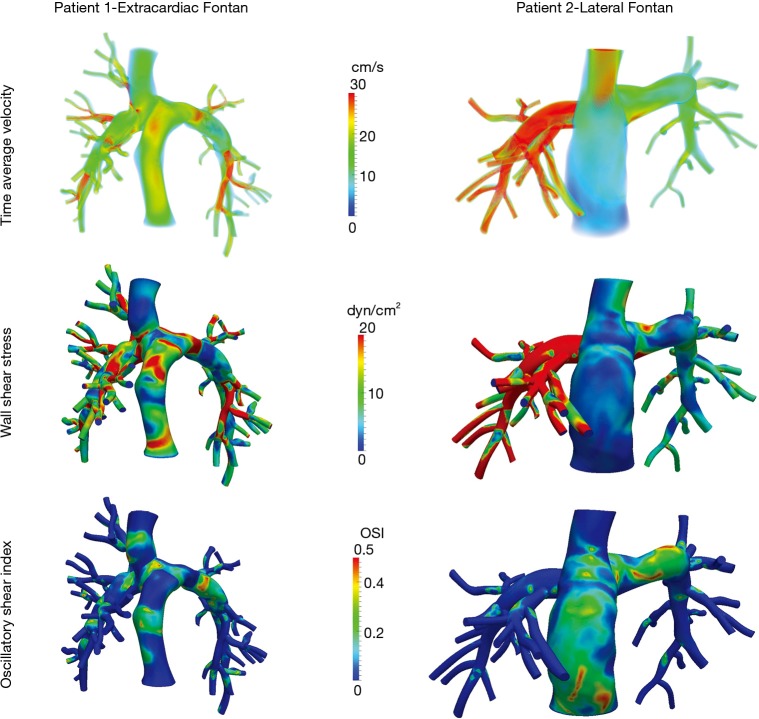
Single ventricle physiology and palliation via the Fontan operation lead to a series of cardiovascular changes. In addition, organs such as the kidneys and liver have been shown to experience insults and subsequent injury. This has led to routine surveillance of patients. We present findings from a small cohort of patients that was deeply phenotyped to illustrate the need for comprehensive evaluation. A cohort of four Fontan patients with fairly high cardiovascular function was recruited 5-10 years post-Fontan. Patients underwent a rigorous clinical work-up after which a research MRI scan was performed during which (I) data were obtained during exercise to evaluate changes in stroke volume during supine exercise and (II) magnetic resonance angiograms with phase-contrast images were obtained for computational modeling of flows through the Fontan circulation at rest. Clinical measures were consistent with a fairly homogeneous high function cohort (peak oxygen consumption >20 mL/kg/min, robust response to exercise, peak ventilatory efficiency below levels associated with heart failure, MR-derived ejection fraction >50%). Liver evaluation did not reveal clear signs of cirrhosis or extensive fibrosis. However, we observed considerable variability (27-162%) in the increase in stroke index with exercise [100%±64% increase, 53.9±17.4 mL/beat m2 (rest), 101.1±20.7 mL/beat m2, (exercise)]. Computational flow modeling at rest in two patients also showed marked differences in flow distribution and shear stress. We report marked differences in both changes in stroke index during an exercise MRI protocol as well as computational flow patterns at rest suggesting different compensation strategies may be associated with high functioning Fontan patients. The observed heterogeneity illustrates the need for deep phenotyping to capture patient-specific adaptive mechanisms.
Keywords: Fontan; exercise; flow modeling; magnetic resonance imaging.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The series “Management of Congenital Heart Disease” was commissioned by the editorial office without any funding or sponsorship. The authors have no conflicts of interest to declare.
Figures