

Study Design of the Phase 3 Sparsentan Versus Irbesartan (DUPLEX) Study in Patients With Focal Segmental Glomerulosclerosis
- PMID: 32274453
- PMCID: PMC7136327
- DOI: 10.1016/j.ekir.2019.12.017
Study Design of the Phase 3 Sparsentan Versus Irbesartan (DUPLEX) Study in Patients With Focal Segmental Glomerulosclerosis
Abstract
Introduction: Focal segmental glomerulosclerosis (FSGS), a histologic lesion in the kidney caused by varied pathophysiological processes, leads to end-stage kidney disease in a large proportion of patients. Sparsentan is a first-in-class orally active compound combining endothelin type A (ETA) receptor blockade with angiotensin II type 1 (AT1) receptor antagonism in a single molecule. A Randomized, Multicenter, Double-Blind, Parallel, Active-Control Study of the Effects of Sparsentan, a Dual Endothelin Receptor and Angiotensin Receptor Blocker, on Renal Outcomes in Patients With Primary FSGS (DUPLEX) study evaluates the long-term antiproteinuric efficacy, nephroprotective potential, and safety profile of sparsentan compared with an AT1 receptor blocker alone in patients with FSGS.
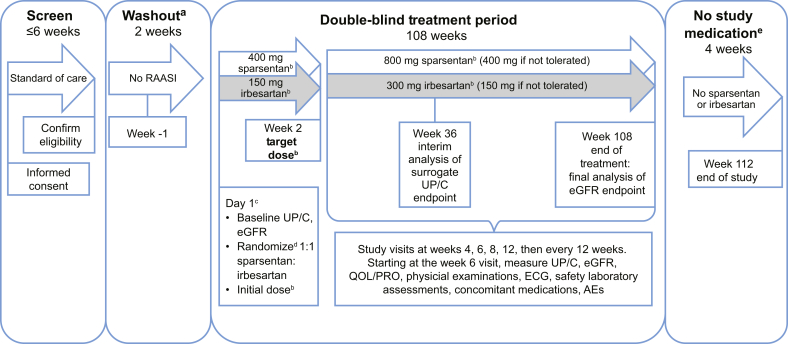
Methods: DUPLEX is a multicenter, international, phase 3, randomized, double-blind, active-controlled study of sparsentan in patients with FSGS. Approximately 300 patients aged 8 to 75 years, inclusive (United States), and 18 to 75 years, inclusive (outside United States) will be randomized 1:1 to daily treatment with sparsentan or irbesartan. After renin-angiotensin-aldosterone system inhibitor washout, treatment will be administered for 108 weeks, with the final assessment at week 112, four weeks after withdrawal of study drug.
Results: The primary endpoint will be the slope of estimated glomerular filtration rate from week 6 to week 108. A novel surrogate efficacy endpoint, the proportion of patients achieving urinary protein-to-creatinine (UP/C) ratio of ≤1.5 g/g and >40% reduction from baseline in UP/C (FSGS partial remission endpoint: FPRE), will be evaluated at a planned interim analysis at week 36. Safety and tolerability of sparsentan will also be assessed.
Conclusion: The phase 3 DUPLEX study will characterize the long-term antiproteinuric efficacy and nephroprotective potential of dual ETA and AT1 receptor blockade with sparsentan in patients with FSGS.
Keywords: angiotensin II type 1 receptor blockade; endothelin type A receptor blockade; focal segmental glomerulosclerosis; irbesartan; proteinuria; sparsentan.
© 2020 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- D'Agati V.D., Kaskel F.J., Falk R.J. Focal segmental glomerulosclerosis. N Engl J Med. 2011;365:2398–2411. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
