

Presurgical Localization of the Primary Sensorimotor Cortex in Gliomas : When is Resting State FMRI Beneficial and Sufficient?
- PMID: 32274518
- PMCID: PMC7943510
- DOI: 10.1007/s00062-020-00879-1
Presurgical Localization of the Primary Sensorimotor Cortex in Gliomas : When is Resting State FMRI Beneficial and Sufficient?
Abstract
Purpose: Functional magnetic resonance imaging (fMRI) has an established role in neurosurgical planning; however, ambiguity surrounds the comparative value of resting and task-based fMRI relative to anatomical localization of the sensorimotor cortex. This study was carried out to determine: 1) how often fMRI adds to prediction of motor risks beyond expert neuroradiological review, 2) success rates of presurgical resting and task-based sensorimotor mapping, and 3) the impact of accelerated resting fMRI acquisitions on network detectability.
Methods: Data were collected at 2 centers from 71 patients with a primary brain tumor (31 women; mean age 41.9 ± 13.9 years) and 14 healthy individuals (6 women; mean age 37.9 ± 12.7 years). Preoperative 3T MRI included anatomical scans and resting fMRI using unaccelerated (TR = 3.5 s), intermediate (TR = 1.56 s) or high temporal resolution (TR = 0.72 s) sequences. Task fMRI finger tapping data were acquired in 45 patients. Group differences in fMRI reproducibility, spatial overlap and success frequencies were assessed with t‑tests and χ2-tests.
Results: Radiological review identified the central sulcus in 98.6% (70/71) patients. Task-fMRI succeeded in 100% (45/45). Resting fMRI failed to identify a sensorimotor network in up to 10 patients; it succeeded in 97.9% (47/48) of accelerated fMRIs, compared to only 60.9% (14/23) of unaccelerated fMRIs ([Formula: see text](2) = 17.84, p < 0.001). Of the patients 12 experienced postoperative deterioration, largely predicted by anatomical proximity to the central sulcus.
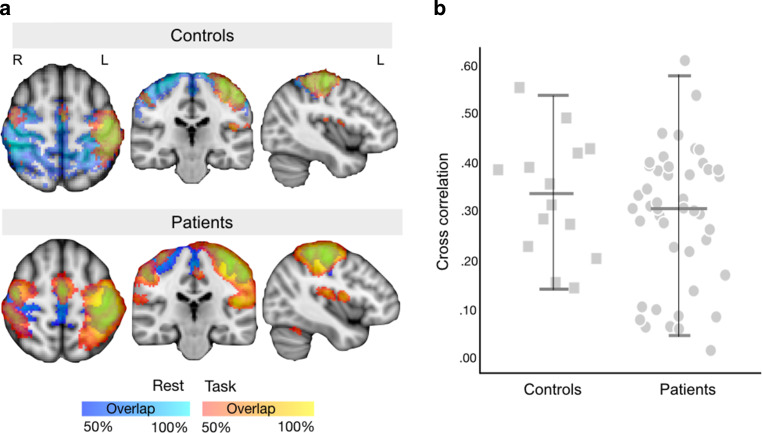
Conclusion: The use of fMRI in patients with residual or intact presurgical motor function added value to uncertain anatomical localization in just a single peri-Rolandic glioma case. Resting fMRI showed high correspondence to task localization when acquired with accelerated sequences but offered limited success at standard acquisitions.
Keywords: ICA; Sensorimotor; Surgery; Task fMRI; Tumor.
Conflict of interest statement
N.L. Voets, P. Plaha, O.P. Jones, P. Pretorius and A. Bartsch declare that they have no competing interests.
Figures



References
-
- Penfield W, Boldrey E. Somatic motor and sensory representation in the cerebral cortex of man as studied by electrical stimulation. Brain. 1937;60:389–443. doi: 10.1093/brain/60.4.389. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
