

COVID-19 Autopsies, Oklahoma, USA
- PMID: 32275742
- PMCID: PMC7184436
- DOI: 10.1093/ajcp/aqaa062
COVID-19 Autopsies, Oklahoma, USA
Erratum in
-
Corrigendum.Am J Clin Pathol. 2020 May 5;153(6):852. doi: 10.1093/ajcp/aqaa070. Am J Clin Pathol. 2020. PMID: 32369558 Free PMC article. No abstract available.
Abstract
Objectives: To report the methods and findings of two complete autopsies of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) positive individuals who died in Oklahoma (United States) in March 2020.
Methods: Complete postmortem examinations were performed according to standard procedures in a negative-pressure autopsy suite/isolation room using personal protective equipment, including N95 masks, eye protection, and gowns. The diagnosis of coronavirus disease 2019 (COVID-19) was confirmed by real-time reverse transcriptase polymerase chain reaction testing on postmortem swabs.
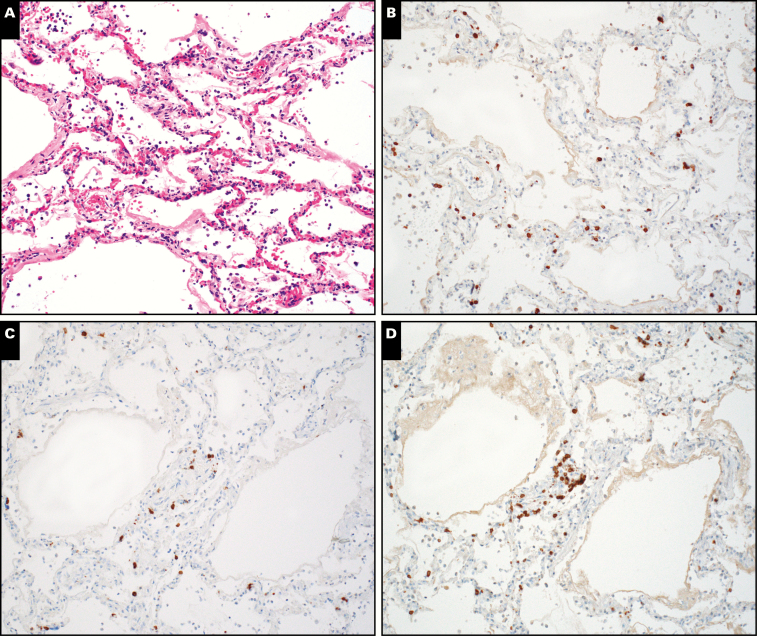
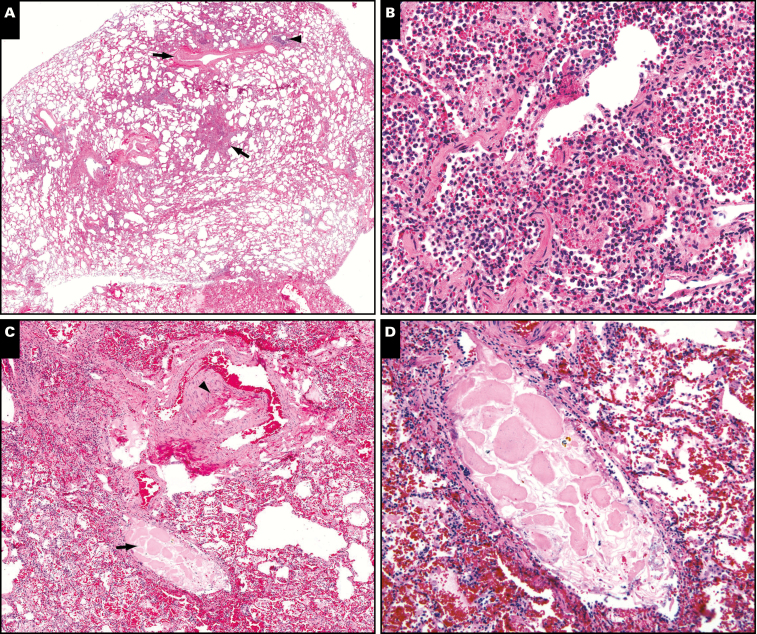
Results: A 77-year-old obese man with a history of hypertension, splenectomy, and 6 days of fever and chills died while being transported for medical care. He tested positive for SARS-CoV-2 on postmortem nasopharyngeal and lung parenchymal swabs. Autopsy revealed diffuse alveolar damage and chronic inflammation and edema in the bronchial mucosa. A 42-year-old obese man with a history of myotonic dystrophy developed abdominal pain followed by fever, shortness of breath, and cough. Postmortem nasopharyngeal swab was positive for SARS-CoV-2; lung parenchymal swabs were negative. Autopsy showed acute bronchopneumonia with evidence of aspiration. Neither autopsy revealed viral inclusions, mucus plugging in airways, eosinophils, or myocarditis.
Conclusions: SARS-CoV-2 testing can be performed at autopsy. Autopsy findings such as diffuse alveolar damage and airway inflammation reflect true virus-related pathology; other findings represent superimposed or unrelated processes.
Keywords: Acute lung injury; Autopsy; COVID-19; Coronavirus; Diffuse alveolar damage; Pulmonary pathology; SARS-CoV-2.
© American Society for Clinical Pathology, 2020. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures




Comment in
-
The role of forensic pathologists in coronavirus disease 2019 infection: The importance of an interdisciplinary research.Med Sci Law. 2020 Jul;60(3):237-238. doi: 10.1177/0025802420927825. Epub 2020 May 21. Med Sci Law. 2020. PMID: 32437227 No abstract available.
References
-
- World Health Organization. Coronavirus disease (COVID-2019) situation reports https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... Accessed April 3, 2020.
-
- Mukhopadhyay S, Mehrad M, Dammert P, et al. Lung biopsy findings in severe pulmonary illness associated with E-cigarette use (vaping). Am J Clin Pathol. 2020;153:30-39. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
