

The Role of Chest Imaging in Patient Management During the COVID-19 Pandemic: A Multinational Consensus Statement From the Fleischner Society
- PMID: 32275978
- PMCID: PMC7138384
- DOI: 10.1016/j.chest.2020.04.003
The Role of Chest Imaging in Patient Management During the COVID-19 Pandemic: A Multinational Consensus Statement From the Fleischner Society
Abstract
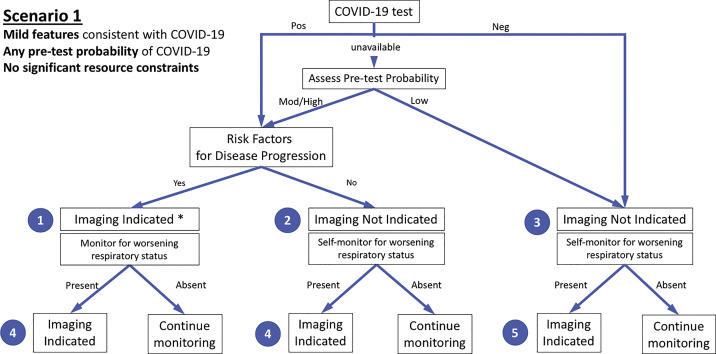
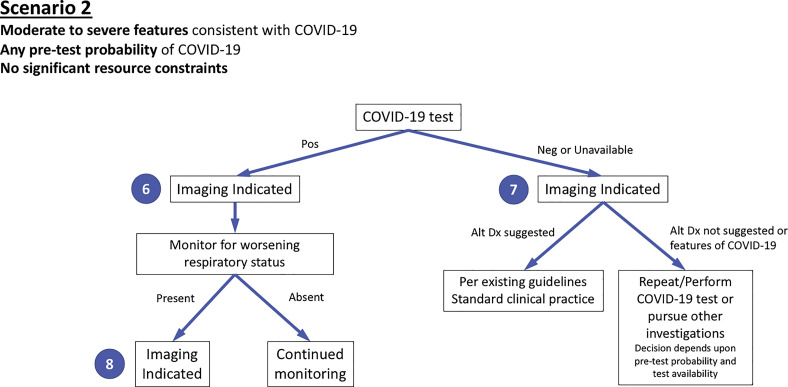
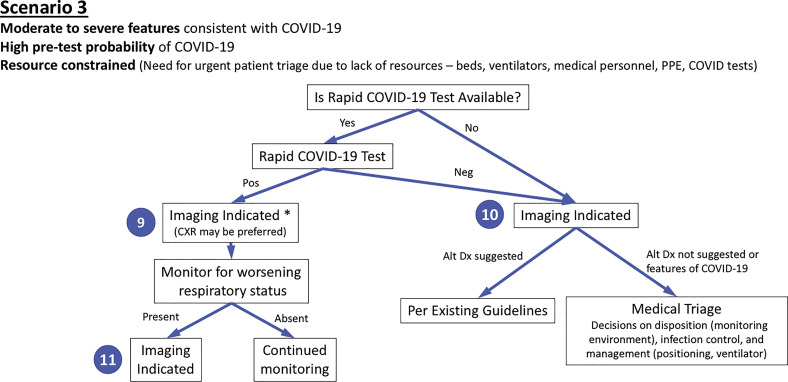
With more than 900,000 confirmed cases worldwide and nearly 50,000 deaths during the first 3 months of 2020, the coronavirus disease 2019 (COVID-19) pandemic has emerged as an unprecedented health care crisis. The spread of COVID-19 has been heterogeneous, resulting in some regions having sporadic transmission and relatively few hospitalized patients with COVID-19 and others having community transmission that has led to overwhelming numbers of severe cases. For these regions, health care delivery has been disrupted and compromised by critical resource constraints in diagnostic testing, hospital beds, ventilators, and health care workers who have fallen ill to the virus exacerbated by shortages of personal protective equipment. Although mild cases mimic common upper respiratory viral infections, respiratory dysfunction becomes the principal source of morbidity and mortality as the disease advances. Thoracic imaging with chest radiography and CT are key tools for pulmonary disease diagnosis and management, but their role in the management of COVID-19 has not been considered within the multivariable context of the severity of respiratory disease, pretest probability, risk factors for disease progression, and critical resource constraints. To address this deficit, a multidisciplinary panel comprised principally of radiologists and pulmonologists from 10 countries with experience managing patients with COVID-19 across a spectrum of health care environments evaluated the utility of imaging within three scenarios representing varying risk factors, community conditions, and resource constraints. Fourteen key questions, corresponding to 11 decision points within the three scenarios and three additional clinical situations, were rated by the panel based on the anticipated value of the information that thoracic imaging would be expected to provide. The results were aggregated, resulting in five main and three additional recommendations intended to guide medical practitioners in the use of chest radiography and CT in the management of COVID-19.
Copyright © 2020 American College of Chest Physicians, published by Elsevier Inc; RSNA. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- World Health Organization Director-General’s opening remarks at the media briefing on COVID-19 - March 11, 2020. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-re...
-
- World Health Organization Coronavirus disease (COVID-19) situation dashboard. https://experience.arcgis.com/experience/685d0ace521648f8a5beeeee1b9125cd
-
- Johns Hopkins University Coronavirus COVID-19 global cases by the Center for Systems Science and Engineering (CSSE) https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
