

First case of COVID-19 complicated with fulminant myocarditis: a case report and insights
- PMID: 32277408
- PMCID: PMC7146072
- DOI: 10.1007/s15010-020-01424-5
First case of COVID-19 complicated with fulminant myocarditis: a case report and insights
Abstract
Background: Coronavirus disease 2019 (COVID-19) has been demonstrated to be the cause of pneumonia. Nevertheless, it has not been reported as the cause of acute myocarditis or fulminant myocarditis.
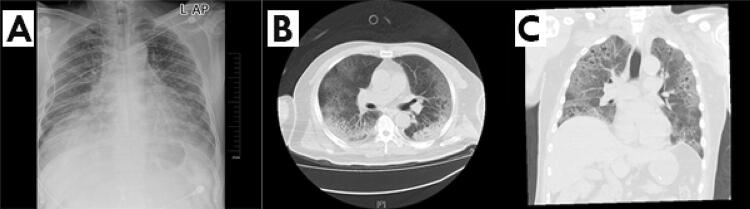
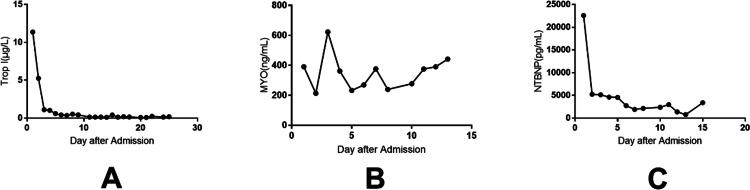
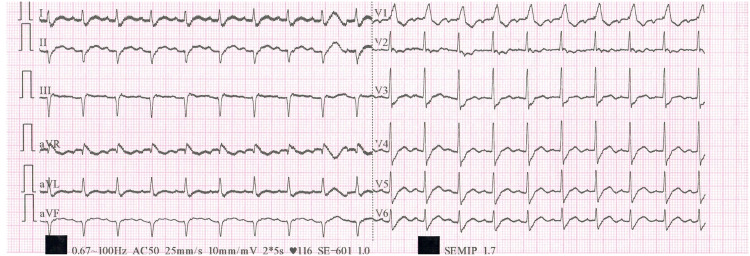
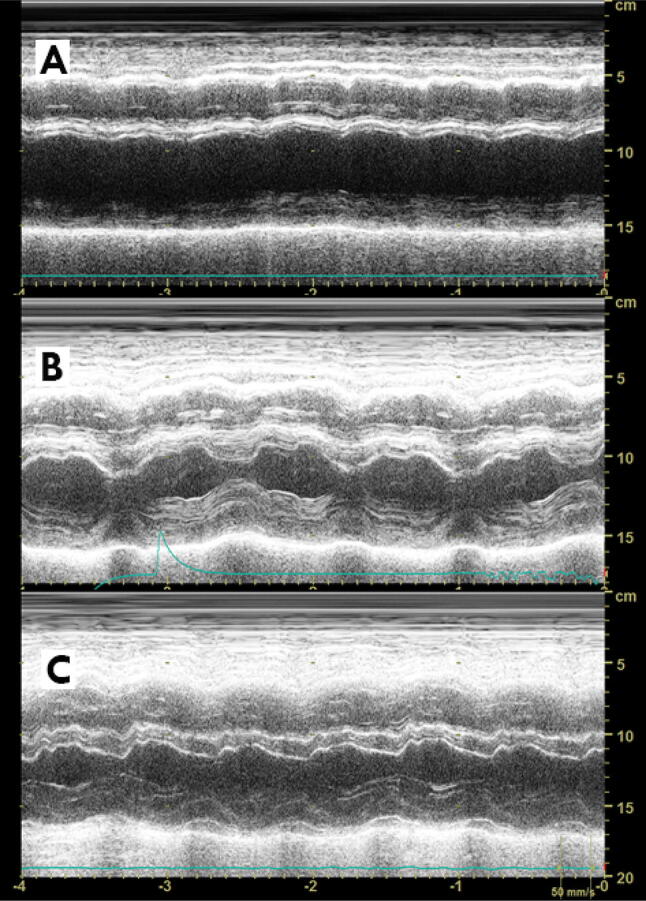
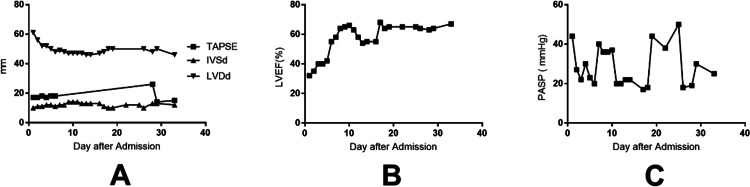
Case presentation: A 63-year-old male was admitted with pneumonia and cardiac symptoms. He was genetically confirmed as having COVID-19 according to sputum testing on the day of admission. He also had elevated troponin I (Trop I) level (up to 11.37 g/L) and diffuse myocardial dyskinesia along with a decreased left ventricular ejection fraction (LVEF) on echocardiography. The highest level of interleukin-6 was 272.40 pg/ml. Bedside chest radiographs showed typical ground-glass changes indicative of viral pneumonia. Laboratory test results for viruses that cause myocarditis were all negative. The patient conformed to the diagnostic criteria of the Chinese expert consensus statement for fulminant myocarditis. After receiving antiviral therapy and mechanical life support, Trop I was reduced to 0.10 g/L, and interleukin-6 was reduced to 7.63 pg/mL. Moreover, the LVEF of the patient gradually recovered to 68%. The patient died of aggravation of secondary infection on the 33rd day of hospitalization.
Conclusion: COVID-19 patients may develop severe cardiac complications such as myocarditis and heart failure. This is the first report of COVID-19 complicated with fulminant myocarditis. The mechanism of cardiac pathology caused by COVID-19 needs further study.
Keywords: COVID-19; Coronavirus; Echocardiography; Fulminant myocarditis; Infection.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there are no conflicts of interest.
Figures
Comment in
-
Glucocorticoid versus immunoglobulin in the treatment of COVID-19-associated fulminant myocarditis.Infection. 2020 Oct;48(5):805-806. doi: 10.1007/s15010-020-01441-4. Epub 2020 May 10. Infection. 2020. PMID: 32388676 Free PMC article. No abstract available.
-
Detailed hemodynamics of fulminant myocarditis caused by COVID-19.Infection. 2020 Dec;48(6):969. doi: 10.1007/s15010-020-01450-3. Epub 2020 May 24. Infection. 2020. PMID: 32449121 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
