

The knowns and unknowns of treatment for alcoholic hepatitis
- PMID: 32277902
- PMCID: PMC7238289
- DOI: 10.1016/S2468-1253(19)30326-7
The knowns and unknowns of treatment for alcoholic hepatitis
Abstract
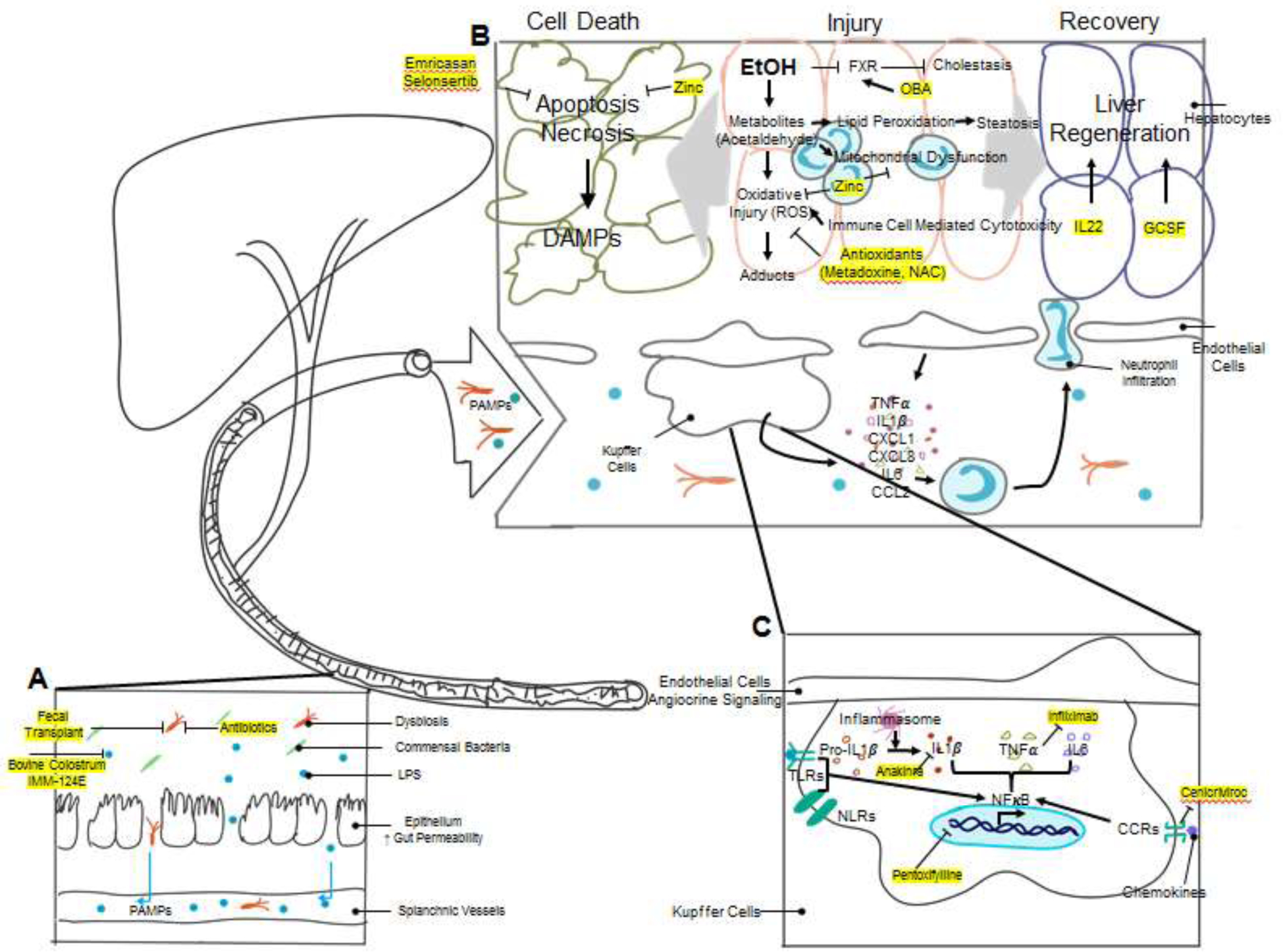
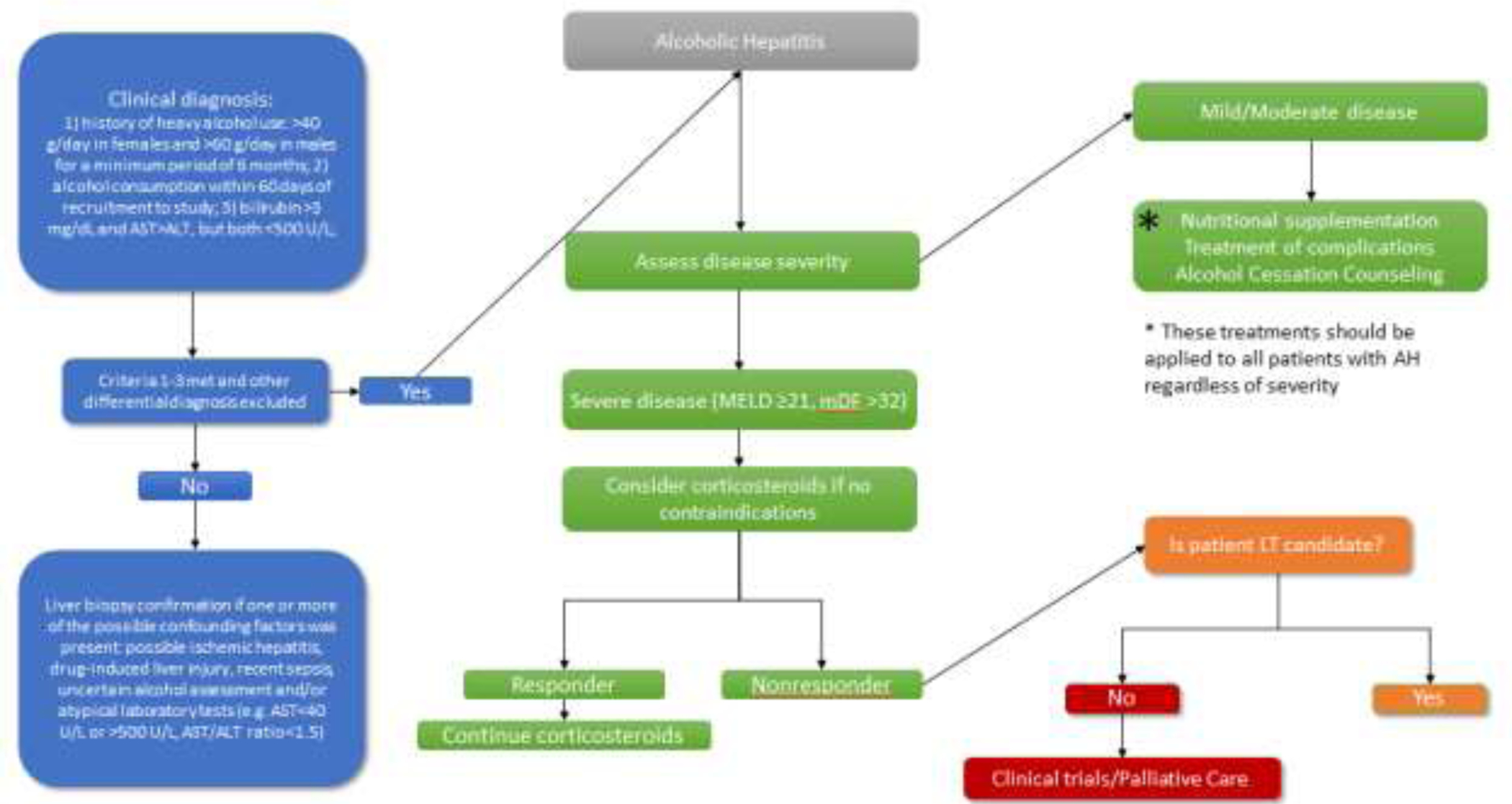
Alcoholic hepatitis is an acute, inflammatory liver disease associated with high morbidity and mortality both in the short term and long term. Alcoholic hepatitis often arises in patients with a background of chronic liver disease and it is characterised by the rapid onset of jaundice and the development of myriad complications. Medical therapy for severe alcoholic hepatitis relies on corticosteroids, which have modest effectiveness. Abstinence from alcohol is critically important in patients with alcoholic hepatitis, but recidivism is high. Because of the absence of effective medical treatments for alcoholic hepatitis and alcohol dependency, there is a pressing need to develop new and effective therapeutics. Supported by promising preliminary and preclinical studies, many ongoing clinical trials of new therapies for alcoholic hepatitis are currently underway and are discussed further in this Series paper.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of Interest Statement
All authors declared no conflict of interest for the work under consideration for publication. Outside submitted work, Prof. V.H.S. reported personal fees from Novartis Pharmaceuticals, Merck Research Laboratories, Afimmune, Ltd., Durect Corporation, Enterome SAB, and Vital Therapies.
Figures
Comment in
-
Use of MELD scores in alcoholic hepatitis.Lancet Gastroenterol Hepatol. 2020 Aug;5(8):720. doi: 10.1016/S2468-1253(20)30194-1. Lancet Gastroenterol Hepatol. 2020. PMID: 32673602 No abstract available.
References
-
- Mathurin P, Duchatelle V, Ramond MJ, Degott C, Bedossa P, Erlinger S, et al. Survival and prognostic factors in patients with severe alcoholic hepatitis treated with prednisolone. Gastroenterology. 1996;110(6):1847–53. - PubMed
-
- Thursz MR, Richardson P, Allison M, Austin A, Bowers M, Day CP, et al. Prednisolone or Pentoxifylline for Alcoholic Hepatitis. New England Journal of Medicine. 2015;372(17):1619–28. - PubMed
-
- McClain RL CaCJ. Alcoholic Liver Disease In: Feldman M MD; Friedman Lawrence S. MD; Brandt Lawrence J. MD, editor. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease. e5 ed: Saunders; 2016. p. 1409–27.
-
- Lieber CS. Alcoholic fatty liver: its pathogenesis and mechanism of progression to inflammation and fibrosis. Alcohol. 2004;34(1):9–19. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
