

Prediction of contralateral breast cancer: external validation of risk calculators in 20 international cohorts
- PMID: 32279280
- PMCID: PMC8380991
- DOI: 10.1007/s10549-020-05611-8
Prediction of contralateral breast cancer: external validation of risk calculators in 20 international cohorts
Abstract
Background: Three tools are currently available to predict the risk of contralateral breast cancer (CBC). We aimed to compare the performance of the Manchester formula, CBCrisk, and PredictCBC in patients with invasive breast cancer (BC).
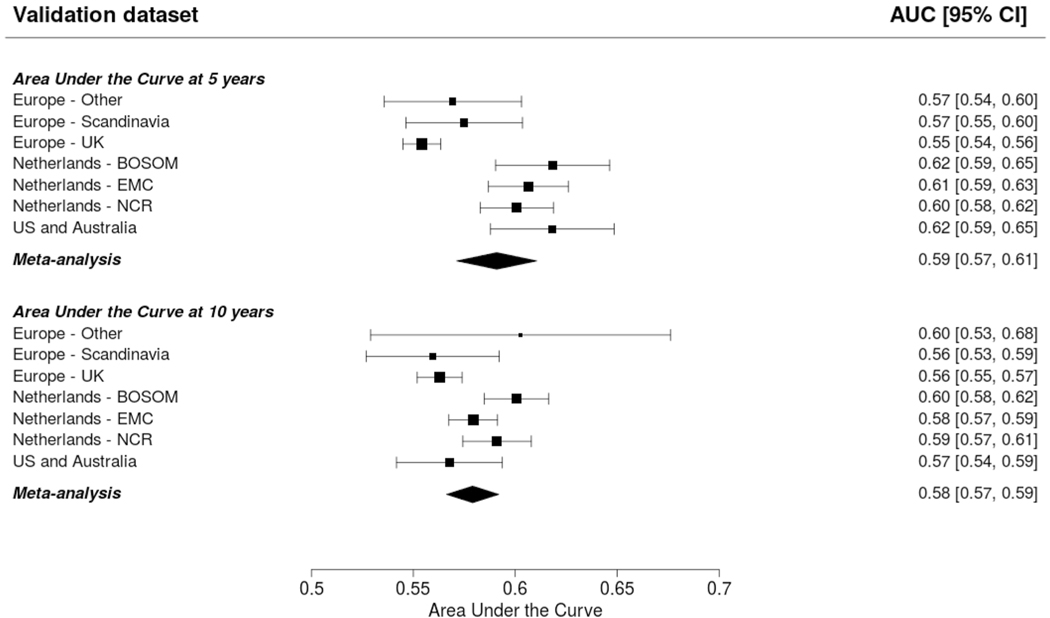
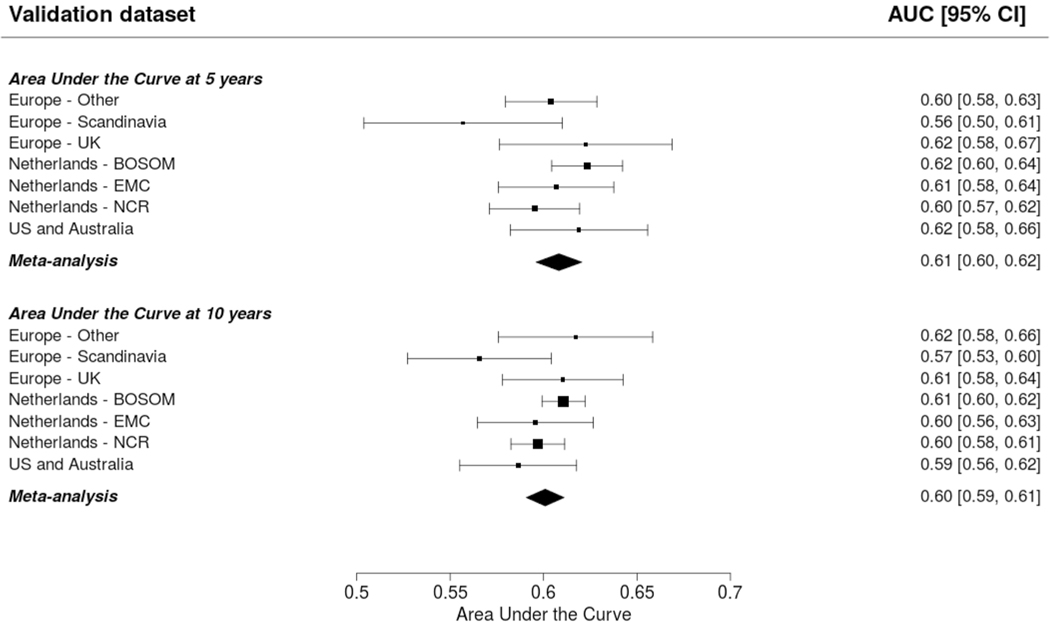
Methods: We analyzed data of 132,756 patients (4682 CBC) from 20 international studies with a median follow-up of 8.8 years. Prediction performance included discrimination, quantified as a time-dependent Area-Under-the-Curve (AUC) at 5 and 10 years after diagnosis of primary BC, and calibration, quantified as the expected-observed (E/O) ratio at 5 and 10 years and the calibration slope.
Results: The AUC at 10 years was: 0.58 (95% confidence intervals [CI] 0.57-0.59) for CBCrisk; 0.60 (95% CI 0.59-0.61) for the Manchester formula; 0.63 (95% CI 0.59-0.66) and 0.59 (95% CI 0.56-0.62) for PredictCBC-1A (for settings where BRCA1/2 mutation status is available) and PredictCBC-1B (for the general population), respectively. The E/O at 10 years: 0.82 (95% CI 0.51-1.32) for CBCrisk; 1.53 (95% CI 0.63-3.73) for the Manchester formula; 1.28 (95% CI 0.63-2.58) for PredictCBC-1A and 1.35 (95% CI 0.65-2.77) for PredictCBC-1B. The calibration slope was 1.26 (95% CI 1.01-1.50) for CBCrisk; 0.90 (95% CI 0.79-1.02) for PredictCBC-1A; 0.81 (95% CI 0.63-0.99) for PredictCBC-1B, and 0.39 (95% CI 0.34-0.43) for the Manchester formula.
Conclusions: Current CBC risk prediction tools provide only moderate discrimination and the Manchester formula was poorly calibrated. Better predictors and re-calibration are needed to improve CBC prediction and to identify low- and high-CBC risk patients for clinical decision-making.
Keywords: Clinical decision-making; Contralateral breast cancer; Risk prediction; Validation.
Conflict of interest statement
Figures
References
-
- Kramer I, Schaapveld M, Oldenburg HSA, Sonke GS, McCool D, van Leeuwen FE, Van de Vijver KK, Russell NS, Linn SC, Siesling S, der Houven M-V, van Oordt CW, Schmidt MK (2019) The influence of adjuvant systemic regimens on contralateral breast cancer risk and receptor subtype. J Natl Cancer Inst. 10.1093/jnci/djz010 - DOI - PubMed
-
- Giardiello D, Steyerberg EW, Hauptmann M, Adank MA, Akdeniz D, Blomqvist C, Bojesen SE, Bolla MK, Brinkhuis M, Chang-Claude J, Czene K, Devilee P, Dunning AM, Easton DF, Eccles DM, Fasching PA, Figueroa J, Flyger H, Garcia-Closas M, Haeberle L, Haiman CA, Hall P, Hamann U, Hopper JL, Jager A, Jakubowska A, Jung A, Keeman R, Kramer I, Lambrechts D, Le Marchand L, Lindblom A, Lubinski J, Manoochehri M, Mariani L, Nevanlinna H, Oldenburg HSA, Pelders S, Pharoah PDP, Shah M, Siesling S, Smit V, Southey MC, Tapper WJ, Tollenaar R, van den Broek AJ, van Deurzen CHM, van Leeuwen FE, van Ongeval C, Van’t Veer LJ, Wang Q, Wendt C, Westenend PJ, Hooning MJ, Schmidt MK (2019) Prediction and clinical utility of a contralateral breast cancer risk model. Breast Cancer Res 21(1):144. 10.1186/s13058-019-1221-1 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
- UM1 CA164973/CA/NCI NIH HHS/United States
- UM1 CA164920/CA/NCI NIH HHS/United States
- 16565/CRUK_/Cancer Research UK/United Kingdom
- R01 CA063464/CA/NCI NIH HHS/United States
- R01 CA132839/CA/NCI NIH HHS/United States
- 16563/CRUK_/Cancer Research UK/United Kingdom
- R01 CA054281/CA/NCI NIH HHS/United States
- U01 CA063464/CA/NCI NIH HHS/United States
- U01 CA098758/CA/NCI NIH HHS/United States
- Z99 CA999999/ImNIH/Intramural NIH HHS/United States
- U01 CA164973/CA/NCI NIH HHS/United States
- R37 CA054281/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
