

A Large Cross-Sectional Survey Study of the Prevalence of Alopecia Areata in the United States
- PMID: 32280257
- PMCID: PMC7131990
- DOI: 10.2147/CCID.S245649
A Large Cross-Sectional Survey Study of the Prevalence of Alopecia Areata in the United States
Abstract
Purpose: Alopecia areata (AA) is an autoimmune disease characterized by the development of non-scarring alopecia. The prevalence is not well known, and estimates vary considerably with no recent estimates in the United States (US). The objective of this study was to define the current AA point prevalence estimate among the general population in the US overall and by severity.
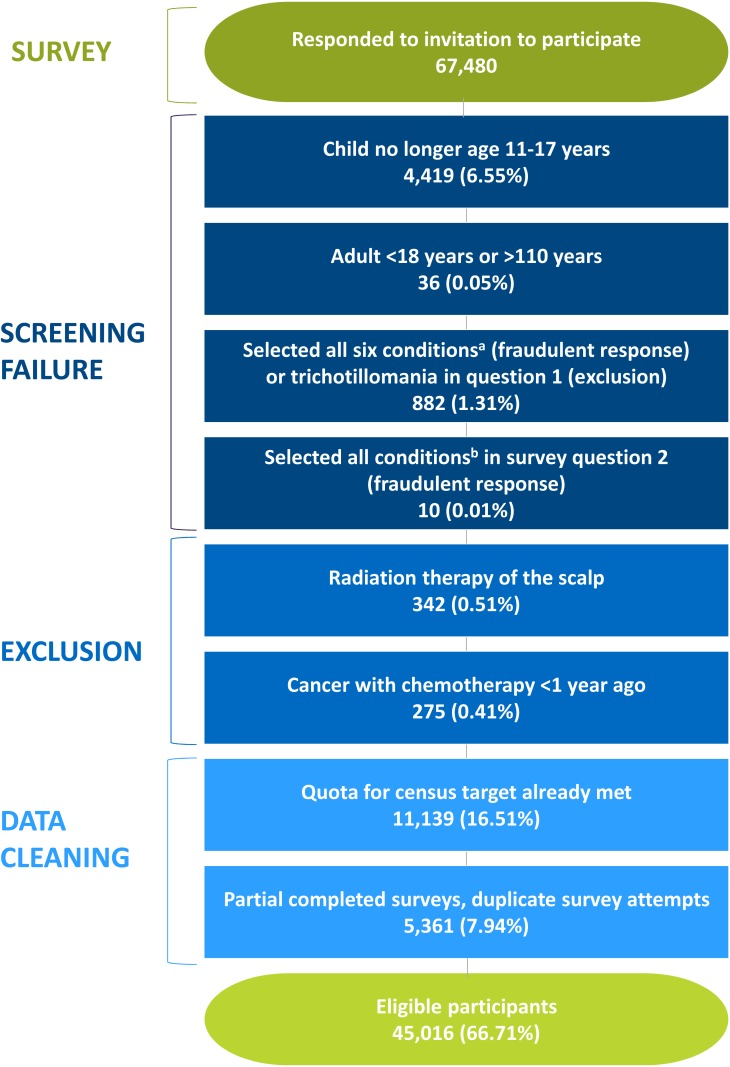
Patients and methods: We administered an online, cross-sectional survey to a representative sample of the US population. Participants self-screening as positive for AA using the Alopecia Assessment Tool (ALTO) also completed the Severity of Alopecia Tool (SALT) to measure the severity of disease as a percent of scalp hair loss. Self-reported AA participants were invited to upload photographs for adjudication of AA by 3 clinicians.
Results: The average age of participants was 43 years. Approximately half of the participants (49.2%) were male, and the majority were white (77.1%) and not of Hispanic origin (93.2%). Among the 511 self-reported AA participants, 104 (20.4%) uploaded photographs for clinician evaluation. Clinician-adjudicated point prevalence of AA was 0.21% (95% CI: 0.17%, 0.25%) overall, 0.12% (95% CI: 0.09%, 0.15%) for "mild" disease (≤50% SALT score), and 0.09% (95% CI: 0.06%, 0.11%) for "moderate to severe" disease (>50% SALT score) with 0.04% (95% CI: 0.02%, 0.06%) for the alopecia totalis/alopecia universalis (100% SALT score) "moderate to severe" subgroup. The average SALT score was 44.4% overall, 8.8% for "mild", and 93.4% for "moderate to severe".
Conclusion: This study suggests that the current AA prevalence in the US is similar to the upper estimates from the 1970s at approximately 0.21% (700,000 persons) with the current prevalence of "moderate to severe" disease at approximately 0.09% (300,000 persons). Given this prevalence and the substantial impact of AA on quality of life, the burden of AA within the US is considerable.
Keywords: Alopecia Assessment Tool; Severity of Alopecia Tool; epidemiology; teledermatology.
© 2020 Benigno et al.
Conflict of interest statement
Michael Benigno, MA, Margarita Udall, MPH, Joseph C. Cappelleri, PhD, Pratibha Chander, MPH, and Elena Peeva, MD, are employees of Pfizer Inc. Michael Benigno reports non-financial support from Covance Market Access Services Inc., during the conduct of the study; Pfizer has an asset in development for the treatment of alopecia areata. Kathryn P. Anastassopoulos, MS, Shoshana R. Daniel, PhD, Jennifer Lapthorn, MS, and Laura Kauffman, MS, are employees of Covance Market Access Services Inc., which was contracted to conduct the study and lead the development of the manuscript. Peter M. Wahl, MLA, MS, ScD was an employee of Covance Market Access Services Inc. during the conduct of the study. Arash Mostaghimi, MPA, MPH, MD is an employee of Brigham and Women’s Hospital, Harvard University and served as a paid consultant to Pfizer. Dr. Mostaghimi also received royalties for licensing of ALTO and participated in the clinical trials for Aclaris, Lilly, Concert, and Incyte. Linda Chen is an independent researcher who was employed at Pfizer during the conduct of the study and is a shareholder of Pfizer stock. The authors report no other conflicts of interest in this work.
Figures
References
LinkOut - more resources
Full Text Sources
