

Pathophysiology and Advanced Hemodynamic Assessment of Cardiogenic Shock
- PMID: 32280412
- PMCID: PMC7137617
- DOI: 10.14797/mdcj-16-1-7
Pathophysiology and Advanced Hemodynamic Assessment of Cardiogenic Shock
Abstract
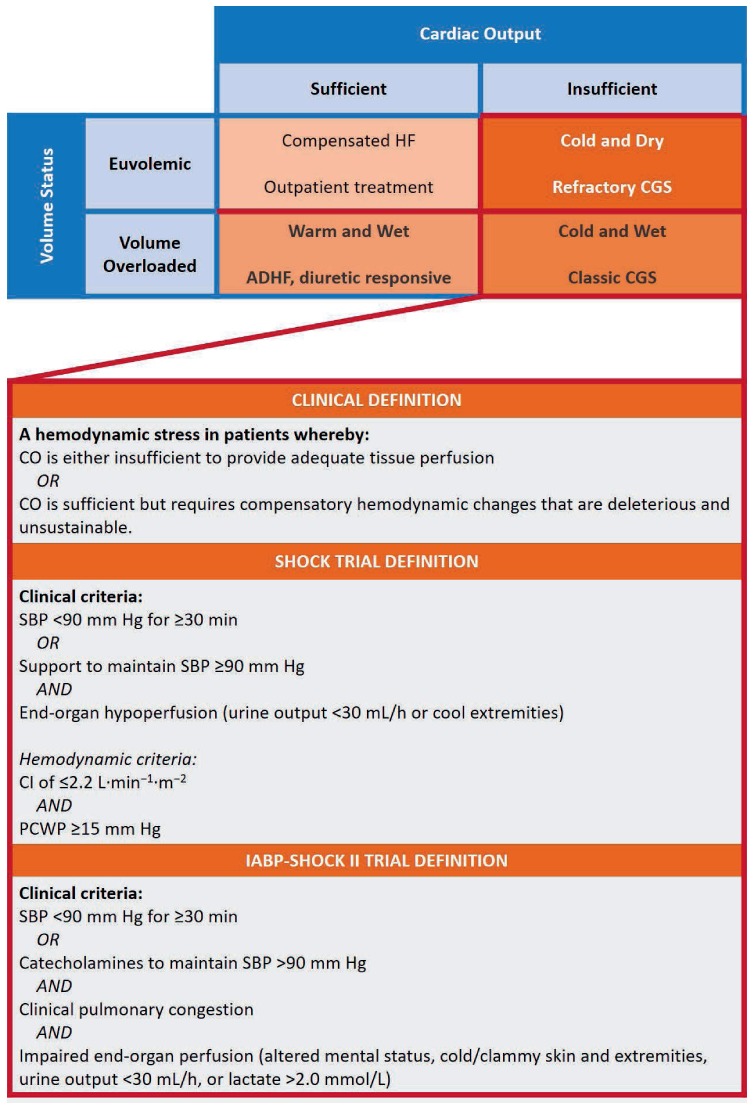
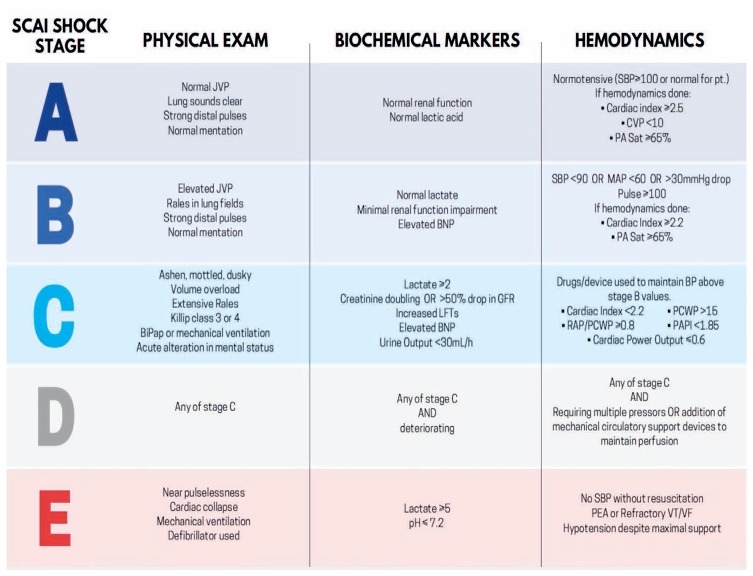
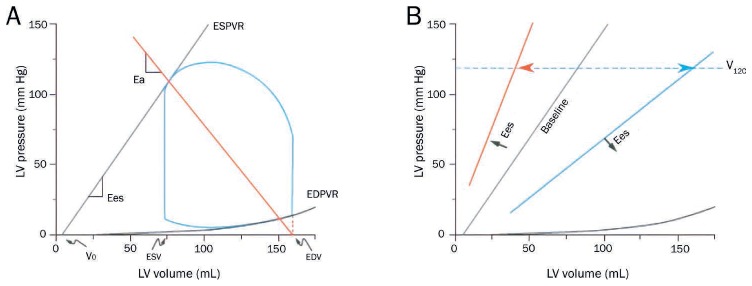
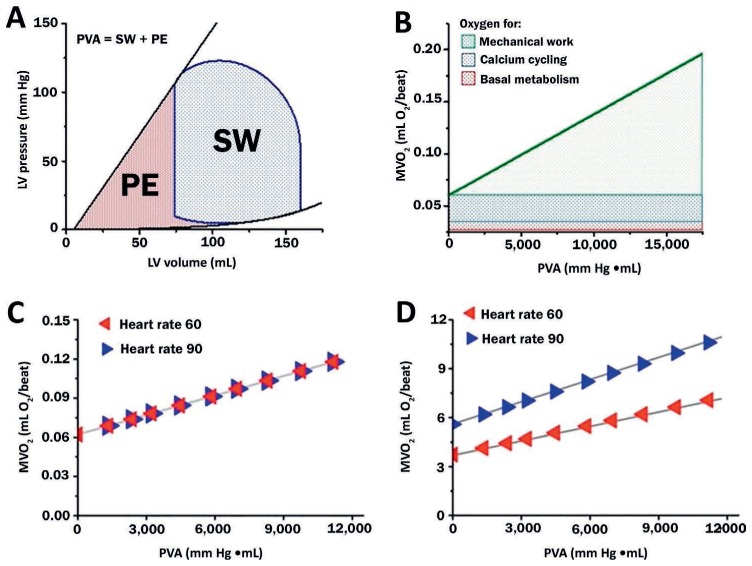
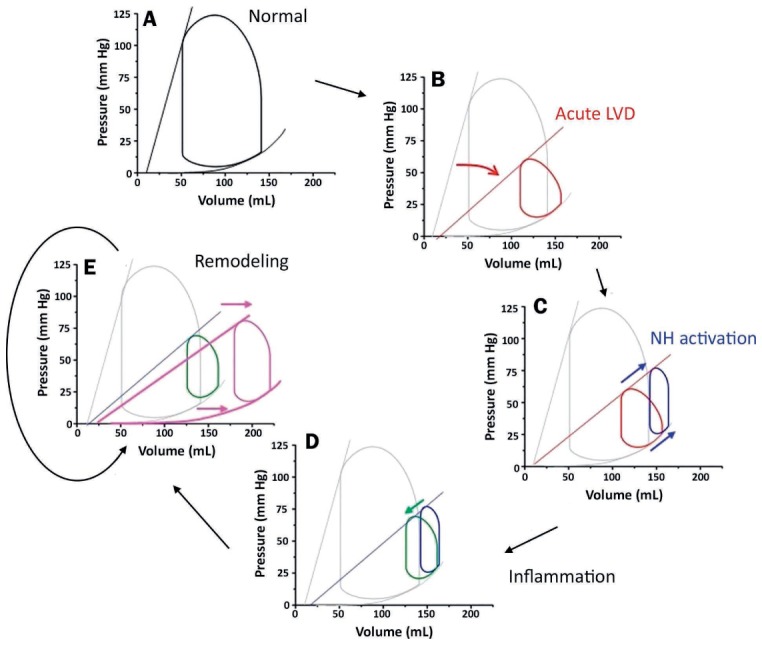
Cardiogenic shock (CGS) is common and highly morbid. According to the National Inpatient Sample, there are more than 100,000 cases per year, and 30-day mortality approaches 50% despite improvements in critical care practices and novel mechanical therapies targeted at restoring normal hemodynamics. This issue aims to enhance clinicians' understanding of CGS, and this review specifically focuses on the underlying pathophysiology. We examine the definition and etiologies of CGS, approaches to risk assessment, and the pressure-volume loop framework that is the foundation for conceptualizing ventricular mechanics, ventricular-vascular interactions, and the derangements observed in CGS. This overview will also contextualize subsequent chapters that discuss nuances of CGS encountered in particular scenarios (ie, post-myocardial infraction, acutely decompensated chronic heart failure, post-cardiac surgery), address pharmacological and mechanical treatments for CGS, and review CGS in a case-based format.
Keywords: cardiogenic shock; hemodynamics; pathogenesis; pressure-volume analysis.
© 2020 Houston Methodist Hospital Houston, Texas.
Conflict of interest statement
Conflict of Interest Disclosure: Dr. Burkhoff conducts research funded by an unrestricted institutional educational grant from Abiomed.
Figures
References
-
- Tsagalou EP, Kanakakis J, Anastasiou-Nana MI et al. Hemodynamic effects of levosimendan in acute myocardial infarction complicated by cardiogenic shock and high systemic vascular resistance. Acute Card Care. 2009;11(2):99–106. - PubMed
-
- Fincke R, Hochman JS, Lowe AM et al. Cardiac power is the strongest hemodynamic correlate of mortality in cardiogenic shock: a report from the SHOCK trial registry. J Am Coll Cardiol. 2004 Jul 21;44(2):340–8. - PubMed
-
- Binanay C, Califf RM, Hasselblad V et al. Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness: the ESCAPE trial. JAMA. 2005 Oct 5;294(13):1625–33. - PubMed
-
- van Diepen S, Katz JN, Albert NM et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation. 2017 Oct 17;136(16):e232–e268. American Heart Association Council on Clinical C, Council on C, Stroke N, Council on Quality of C, Outcomes R and Mission L. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
