

Physiological Concepts of Cardiogenic Shock Using Pressure-Volume Loop Simulations: A Case-Based Review
- PMID: 32280417
- PMCID: PMC7137624
- DOI: 10.14797/mdcj-16-1-43
Physiological Concepts of Cardiogenic Shock Using Pressure-Volume Loop Simulations: A Case-Based Review
Abstract
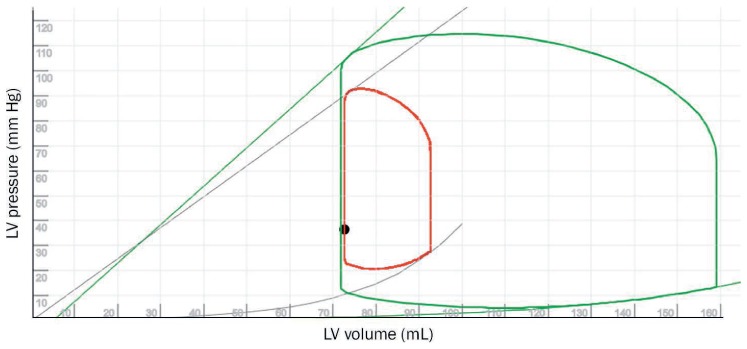
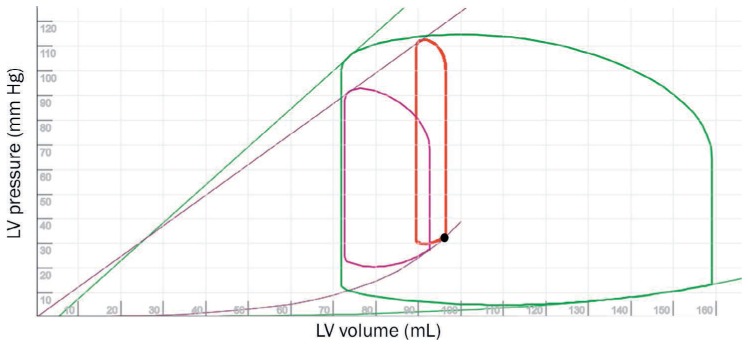
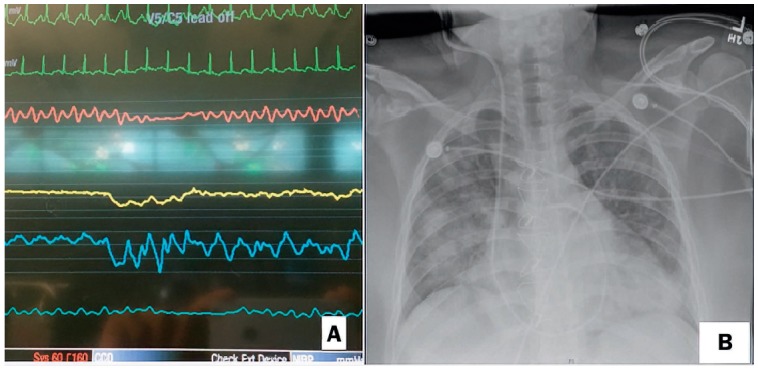
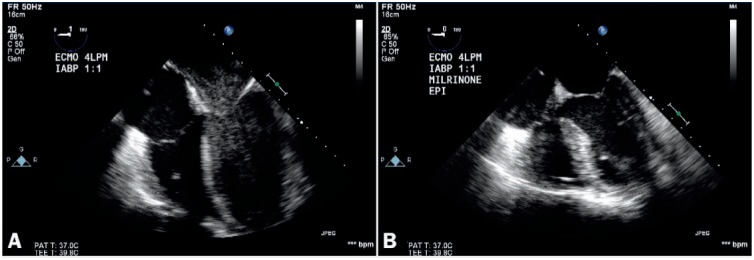
Cardiogenic shock (CS) is a complex syndrome of end-organ hypoperfusion that requires timely and thorough decision making. While many pathophysiologic and technical principles have been delineated in this issue, the purpose of this case-based report is to reflect upon some of these principles in the context of real-life scenarios. Given the obvious lacuna of evidence-based recommendations in CS, the authors provide a rationale for their decision-making process. The first case is a young post-heart-transplant patient with graft failure who was in a state of biventricular failure and restrictive physiology and required acute mechanical circulatory support (MCS). The second case is a patient who suffered a mechanical complication after experiencing an acute myocardial infarction that required MCS.
Keywords: cardiogenic shock; heart failure; mechanical support devices; pressure volume loop physiology.
© 2020 Houston Methodist Hospital Houston, Texas.
Conflict of interest statement
Conflict of Interest Disclosure: The authors have completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
Figures
References
-
- Harvi Online [Internet] Burkhoff D, Dickstein ML, Schleicher T. c2020 [cited 2019 Dec 30]. Available from: https://harvi.online.
-
- Kapur NK, Esposito ML, Bader Y et al. Mechanical Circulatory Support Devices for Acute Right Ventricular Failure. Circulation. 2017 Jul 18;136(3):314–26. - PubMed
-
- Pappalardo F, Schulte C, Pieri M et al. Concomitant implantation of Impella® on top of veno-arterial extracorporeal membrane oxygenation may improve survival of patients with cardiogenic shock. Eur J Heart Fail. 2017 Mar;19(3):404–12. - PubMed
-
- Kaneko D, Takahashi M, Fukutomi M, Funayama H, Kario K. Additional Use of a 6F Intra-Aortic Balloon Pump on Extracorporeal Membrane Oxygenation Was Effective in a Patient with Cardiogenic Shock with Low Pulse Pressure. Int Heart J. 2019 Sep 27;60(5):1184–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
