

Effect of an Enhanced Paramedic Acute Stroke Treatment Assessment on Thrombolysis Delivery During Emergency Stroke Care: A Cluster Randomized Clinical Trial
- PMID: 32282015
- PMCID: PMC7154959
- DOI: 10.1001/jamaneurol.2020.0611
Effect of an Enhanced Paramedic Acute Stroke Treatment Assessment on Thrombolysis Delivery During Emergency Stroke Care: A Cluster Randomized Clinical Trial
Abstract
Importance: Rapid thrombolysis treatment for acute ischemic stroke reduces disability among patients who are carefully selected, but service delivery is challenging.
Objective: To determine whether an enhanced Paramedic Acute Stroke Treatment Assessment (PASTA) intervention increased hospital thrombolysis rates.
Design, setting, and participants: This multicenter, cluster randomized clinical trial took place between December 2015 and July 2018 in 3 ambulance services and 15 hospitals. Clusters were paramedics based within ambulance stations prerandomized to PASTA or standard care. Patients attended by study paramedics were enrolled after admission if a hospital specialist confirmed a stroke and paramedic assessment started within 4 hours of onset. Allocation to PASTA or standard care reflected the attending paramedic's randomization status.
Interventions: The PASTA intervention included additional prehospital information collection, a structured hospital handover, practical assistance up to 15 minutes after handover, a predeparture care checklist, and clinician feedback. Standard care reflected national guidelines.
Main outcomes and measures: Primary outcome was the proportion of patients receiving thrombolysis. Secondary outcomes included time intervals and day 90 health (with poor status defined as a modified Rankin Score >2, to represent dependency or death).
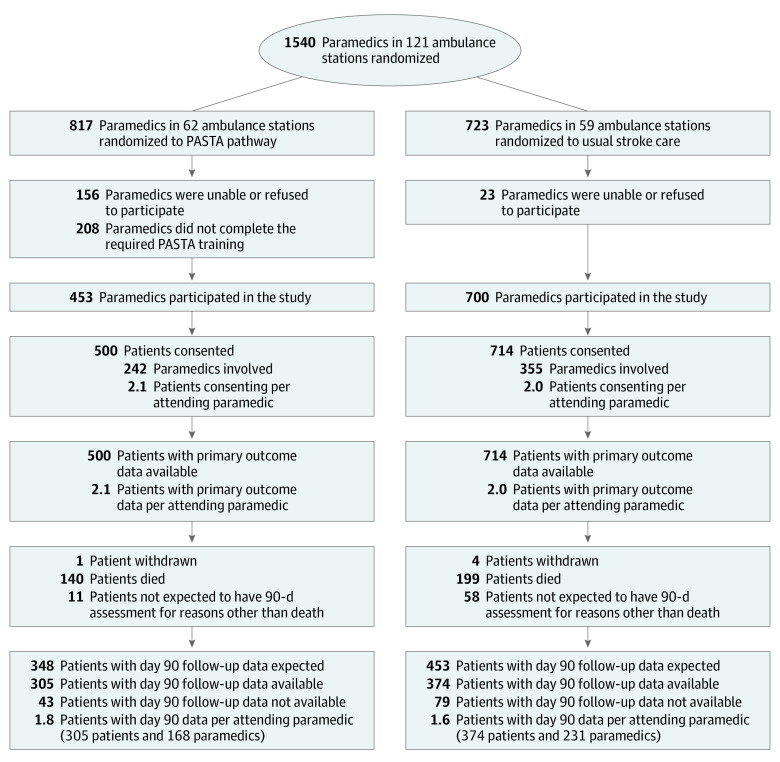
Results: A total of 11 478 patients were screened following ambulance transportation; 1391 were eligible and approached, but 177 did not consent. Of 1214 patients enrolled (mean [SD] age, 74.7 [13.2] years; 590 women [48.6%]), 500 were assessed by 242 paramedics trained in the PASTA intervention and 714 were assessed by 355 paramedics continuing with standard care. The paramedics trained in the PASTA intervention took a mean of 13.4 (95% CI, 9.4-17.4) minutes longer (P < .001) to complete patient care episodes. There was less thrombolysis among the patients in the PASTA group, but this was not significant (PASTA group, 197 of 500 patients [39.4%] vs the standard care group, 319 of 714 patients [44.7%]; adjusted odds ratio, 0.81 [95% CI, 0.61-1.08]; P = .15). Time from a paramedic on scene to thrombolysis was a mean of 8.5 minutes longer in the PASTA group (98.1 [37.6] minutes) vs the standard care group (89.4 [31.1] minutes; P = .01). Poor health outcomes did not differ significantly but occurred less often among patients in the PASTA group (313 of 489 patients [64.0%]) vs the standard care group (461 of 690 patients [66.8%]; adjusted odds ratio, 0.86 [95% CI, 0.60-1.20]; P = .39).
Conclusions and relevance: An enhanced paramedic assessment did not facilitate thrombolysis delivery. The unexpected combination of thrombolysis and health outcomes suggests possible alternative influences on treatment decisions by the intervention, requiring further evaluation.
Trial registration: ISRCTN Registry Identifier: ISRCTN12418919.
Conflict of interest statement
Figures


References
-
- School of Population Health and Environmental Studies King’s College London Sentinel Stroke National Audit Programme. Published 2020. Accessed March 5, 2020. https://www.strokeaudit.org
-
- Lorenzano S, Ahmed N, Tatlisumak T, et al. ; SITS Investigators . Within-day and weekly variations of thrombolysis in acute ischemic stroke: results from safe implementation of treatments in stroke-international stroke thrombolysis register. Stroke. 2014;45(1):176-184. doi: 10.1161/STROKEAHA.113.002133 - DOI - PubMed
