Assessment of an Unplanned Extubation Bundle to Reduce Unplanned Extubations in Critically Ill Neonates, Infants, and Children
- PMID: 32282029
- PMCID: PMC7154960
- DOI: 10.1001/jamapediatrics.2020.0268
Assessment of an Unplanned Extubation Bundle to Reduce Unplanned Extubations in Critically Ill Neonates, Infants, and Children
Abstract
Importance: Unplanned extubations (UEs) in children contribute to significant morbidity and mortality, with an arbitrary benchmark target of less than 1 UE per 100 ventilator days. However, there have been no multicenter initiatives to reduce these events.
Objective: To determine if a multicenter quality improvement initiative targeting all intubated neonatal and pediatric patients is associated with a reduction in UEs and morbidity associated with UE events.
Design, setting, and participants: This multicenter quality improvement initiative enrolled patients from pediatric, neonatal, and cardiac intensive care units (ICUs) in 43 participating children's hospitals from March 2016 to December 2018. All patients with an endotracheal tube requiring mechanical ventilation were included in the study.
Interventions: Participating hospitals implemented a quality improvement bundle to reduce UEs, which included standardized anatomic reference points and securement methods, protocol for high-risk situations, and multidisciplinary apparent cause analyses.
Main outcomes and measures: The main outcome measures for this study included bundle compliance with each factor tested and UE rates on the center level and on the cohort level.
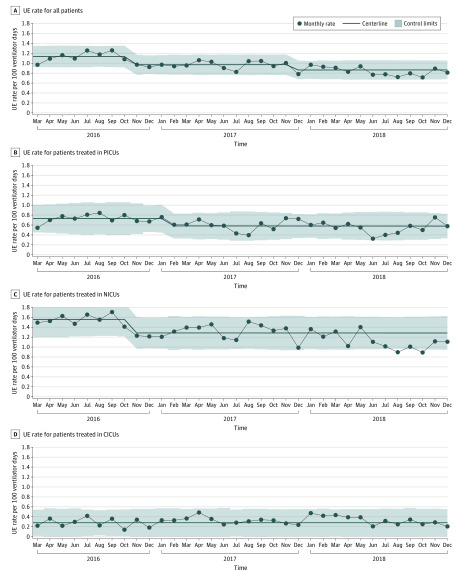
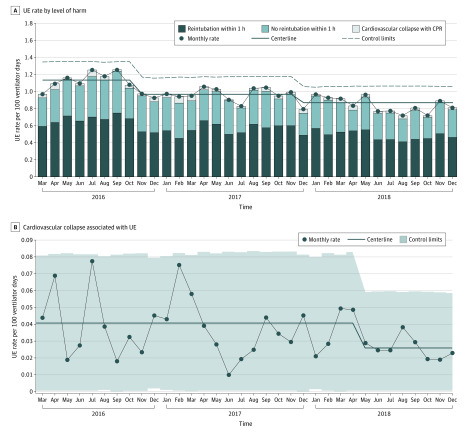
Results: Among the 43 children's hospitals, the quality improvement initiative was associated with an aggregate 24.1% reduction in UE events, from a baseline rate of 1.135 UEs per 100 ventilator days to 0.862 UEs per 100 ventilator days. Across ICU settings studied, the pediatric ICU and neonatal ICU demonstrated centerline shifts, with an absolute reduction in events of 20.6% (from a baseline rate of 0.729 UEs per 100 ventilator days to 0.579 UEs per 100 ventilator days) and 17.6% (from a baseline rate of 1.555 UEs per 100 ventilator days to 1.282 UEs per 100 ventilator days), respectively. Most UEs required reintubation within 1 hour (mean of 120 of 206 events per month [58.3%]), followed by UEs that did not require reintubation (mean of 78 of 206 events per month [37.9%]) and UEs that resulted in cardiovascular collapse (mean of 8 of 206 events per month [3.9%]). Cardiovascular collapse events represented the most significant consequence of UE studied, and the collaborative reduced these UE events by 36.6%, from a study baseline rate of 0.041 UEs per 100 ventilator days to 0.026 UEs per 100 ventilator days.
Conclusions and relevance: This multicenter quality improvement initiative was associated with a reduction in UEs across different pediatric populations in diverse settings. A significant reduction in event rate and rate of harm (cardiovascular collapse) was observed, which was sustained over the time course of the intervention. This quality improvement process and UE bundle may be considered standard of care for pediatric hospitals in the future.
Conflict of interest statement
Figures