

Mature Follicle Count and Multiple Gestation Risk Based on Patient Age in Intrauterine Insemination Cycles With Ovarian Stimulation
- PMID: 32282611
- PMCID: PMC7183886
- DOI: 10.1097/AOG.0000000000003795
Mature Follicle Count and Multiple Gestation Risk Based on Patient Age in Intrauterine Insemination Cycles With Ovarian Stimulation
Abstract
Objective: To estimate the risk of a multiple gestation pregnancy in ovarian stimulation intrauterine insemination (IUI) cycles when stratified by patient age and mature follicle number.
Methods: We conducted a retrospective cohort study at a single private practice fertility center of IUI cycles performed from 2004 to 2017. Intervention(s) were ovarian stimulation and IUI if postwash total motile sperm count was more than 8 million. Mature follicles were defined as 14 mm or more as measured on the day of ovulation trigger. Main outcomes and measures were rates of clinical pregnancy and multiple gestation.
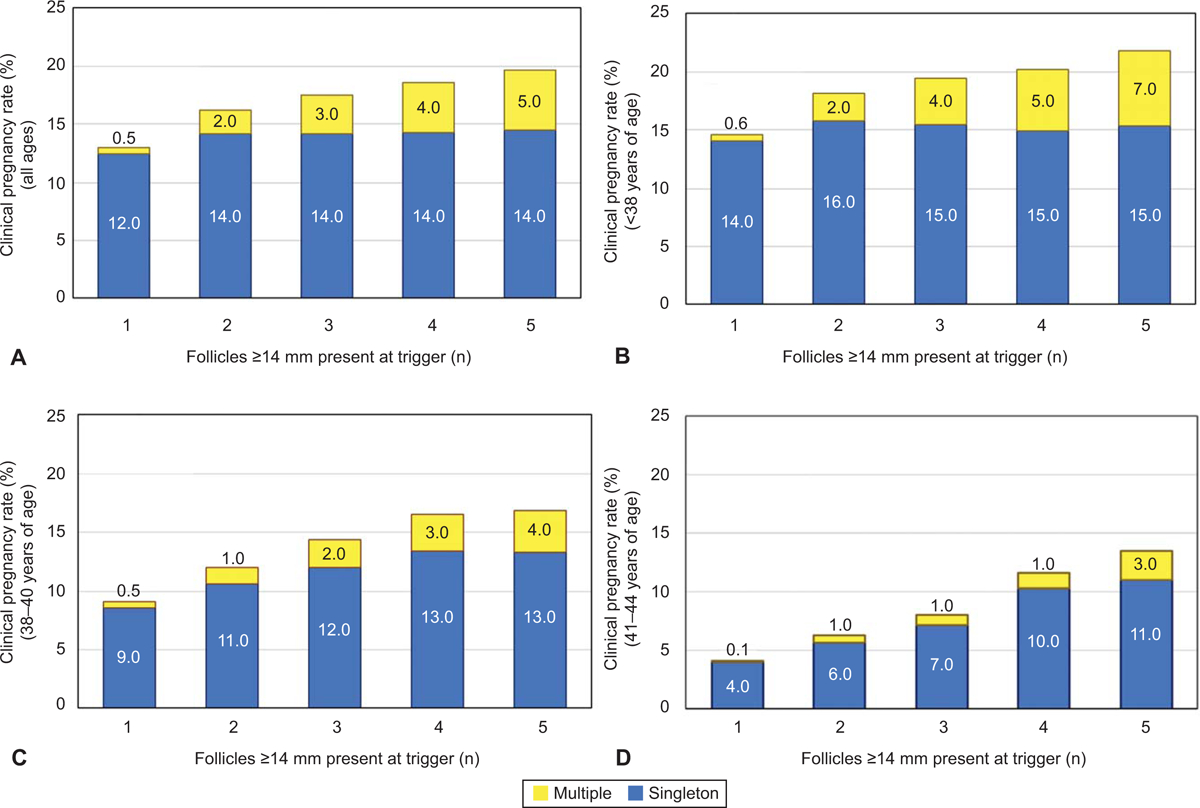
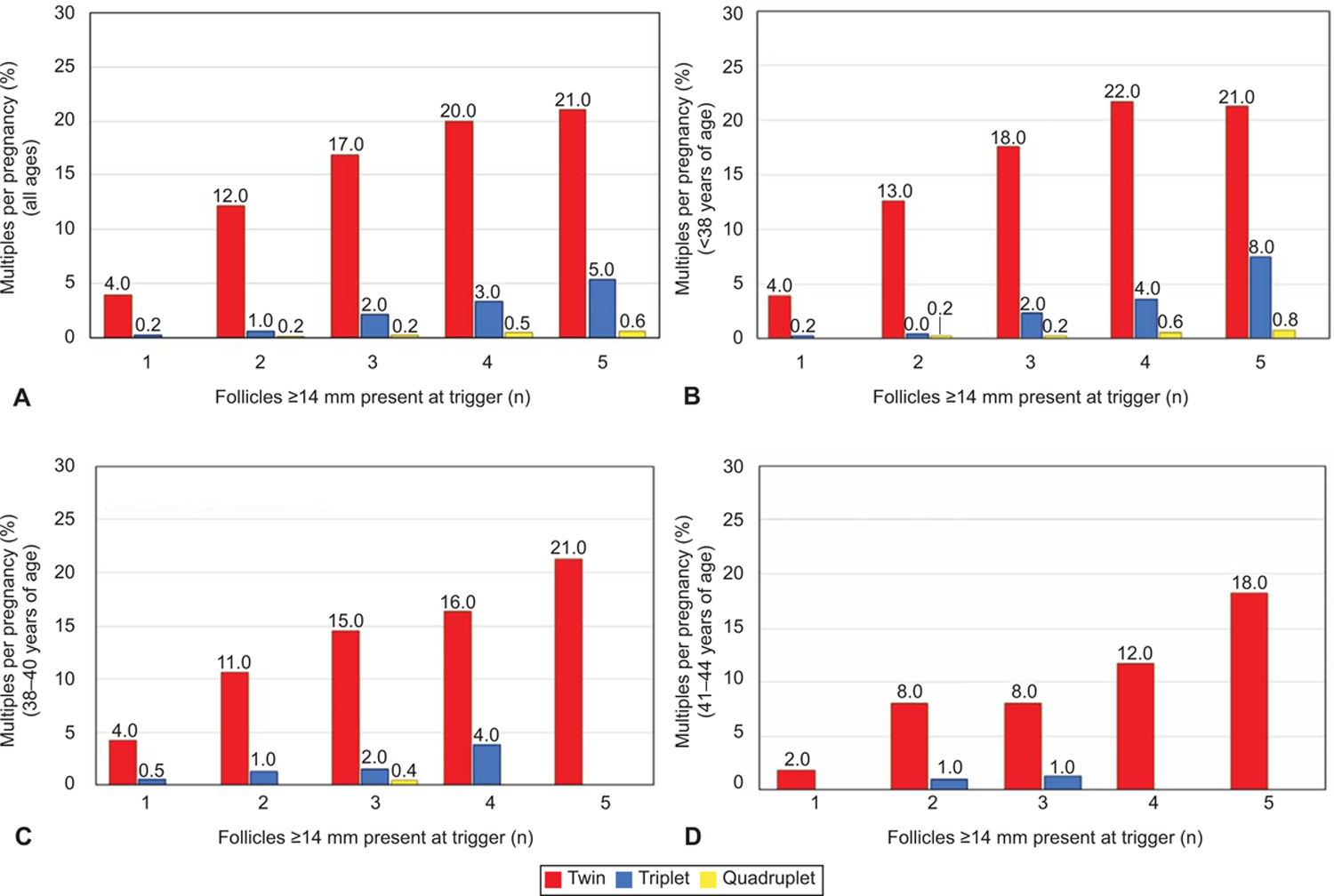
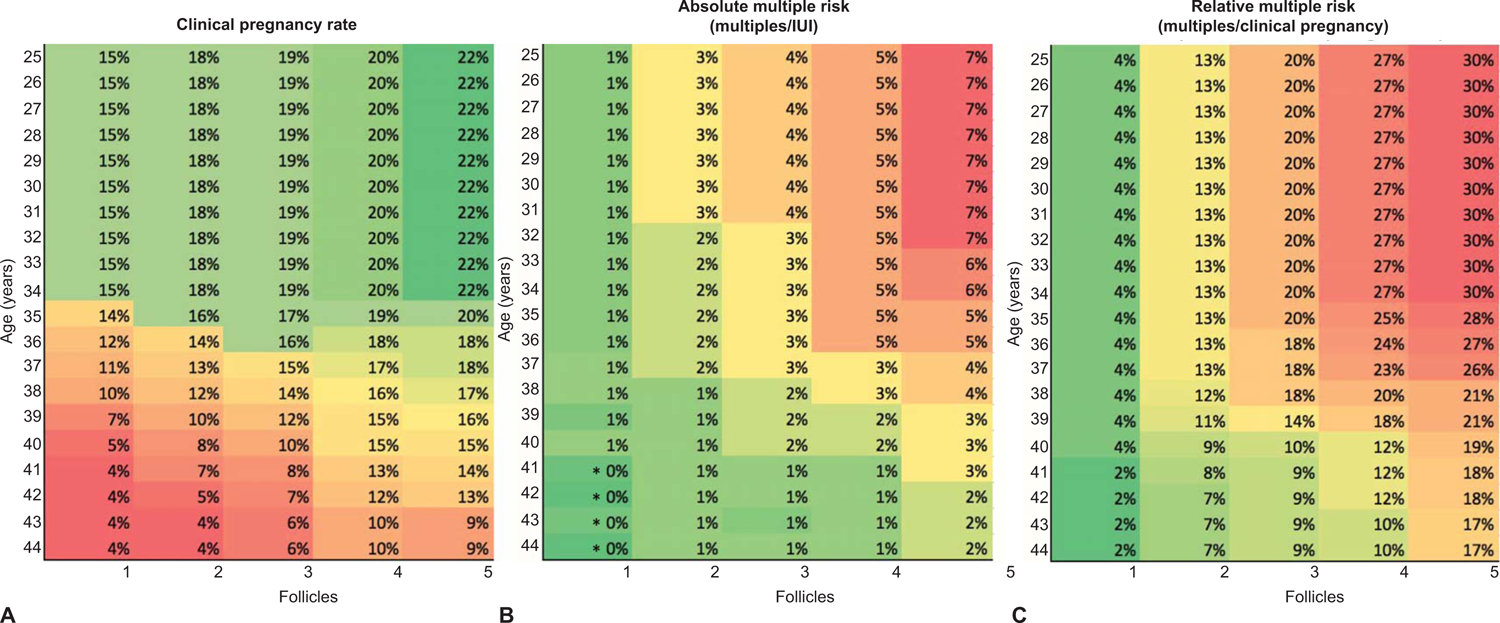
Results: We identified 24,649 women who underwent a total of 50,473 IUI cycles. Increasing the number of mature follicles from one to five at the time of IUI in women younger than age 38 years increased the clinical pregnancy rate from 14.6% to 21.9% (adjusted odds ratio [aOR] 1.6, 95% CI 1.4-1.9), almost entirely from a marked increase in multiple gestations per cycle from 0.6% to 6.5% (aOR 9.9, 95% CI 6.9-14.2). There was little increase in singleton pregnancies per IUI (14.1-16.4%) regardless of mature follicle number. The per-pregnancy twin and higher-order multiple gestation risk significantly increased (3.9-23.3%, P<.01 and 0.2-10.6%, P<.01, respectively) when comparing one with five mature follicles present at the time of IUI (P<.01). In women younger than age 38 years with more than three follicles present, more than one quarter of all pregnancies were multiples. Similar findings occurred in women aged 38-40 years. In women older than age 40 years, up to four follicles tripled the odds of pregnancy (aOR 3.1, 95% CI 2.1-4.5) while maintaining a less than 12% risk of multiple gestation per pregnancy and a 1.0% absolute risk of multiples.
Conclusion: Caution should be used in proceeding with IUI after ovarian stimulation when there are more than two mature follicles in women younger than age 40 years owing to the substantially increased risk of multiple gestation without an improved chance of singleton clinical pregnancy.
Conflict of interest statement
Financial Disclosure
Micah Hill served on the advisory board of and received personal fees from Ohana Biosciences. Kevin S. Richter disclosed that he was a paid consultant for EMD Serono. The other authors did not report any potential conflicts of interest.
Each author has confirmed compliance with the journal’s requirements for authorship.
Figures
Comment in
-
Too Much of a Good Thing: Multiple Gestations With Intrauterine Insemination.Obstet Gynecol. 2020 May;135(5):1003-1004. doi: 10.1097/AOG.0000000000003849. Obstet Gynecol. 2020. PMID: 32282590 No abstract available.
References
-
- D’Alton ME, Mercer BM. Antepartum management of twin gestation: ultrasound. Clin Obstet Gynecol 1990;33:42–51. - PubMed
-
- Adams DM, Sholl JS, Haney EI, Russell TL, Silver RK. Perinatal outcome associated with outpatient management of triplet pregnancy. Am J Obstet Gynecol 1998;178:843–7. - PubMed
-
- Multifetal gestations: twin, triplet, and higher-order multifetal pregnancies. Practice Bulletin No. 169. American College of Obstetricians and Gynecologists. Obstet Gynecol 2016;128:e131–46. - PubMed
-
- Martin JA, MacDorman MF, Mathews TJ. Triplet births: trends and outcomes, 1971–94. Vital Health Stat 21 1997:1–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
