

Transesophageal and intracardiac ultrasound in arrhythmogenic right ventricular dysplasia/cardiomyopathy: Two case reports
- PMID: 32282747
- PMCID: PMC7220632
- DOI: 10.1097/MD.0000000000019817
Transesophageal and intracardiac ultrasound in arrhythmogenic right ventricular dysplasia/cardiomyopathy: Two case reports
Abstract
Rationale: Two-dimensional echocardiography (2D echo) is a major tool for the diagnosis of Arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C). However 2D echo can skip regional localized anomalies of the right ventricular wall. We aimed to determine whether transesophageal and intracardiac ultrasound can provide additional information, on the right ventricular abnormalities compared to 2D echo.
Patient concerns: Case 1 is a 30-year-old patient that presented in the Emergency Department with multiple episodes of fast monomorphic ventricular tachycardia (VT) manifested by palpitations and diziness. Case 2 is a 65-year-old patient that also presented with episodes of ventircular tachycardia associated with low blood pressure.
Diagnosis: Both patients had a clear diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy confirmed by cardiac magnetic resonance imaging.
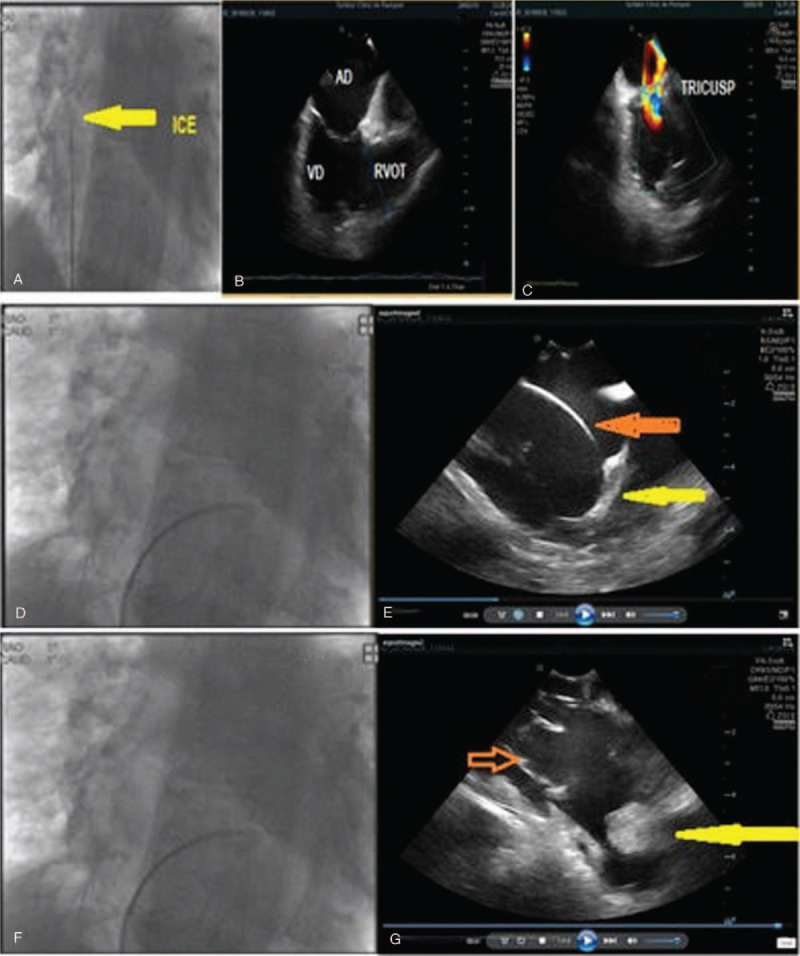
Intervention: In both patients transesophageal and intracardiac ultrasound was performed, which brought more information on the diagnosis of ARVD/C compared to transthoracic echocardiograpy.
Outcomes: The first patient was implanted with an internal cardiac defibrillator and treated with Sotalol for VT recurrences. He presented episodes of VT during follow-up, treated with antitachycardia pacing. The second patient was implanted with an internal cardiac defibrillator and treated with Sotalol without any VT recurrence at 18 month-follow-up.
Lessons: Transesophageal echocardiography and intracardiac echocardiography can provide additional information on small, focal structural abnormalities in patients with ARVD/C: bulges, saculations, aneurysms with or without associated thrombus, partial or complete loss of trabeculations and hypertrophy of the moderator band. These changes are particularly important in cases with "concealed" form of the disease in which no morphological abnormalities are evident in transthoracic echocardiograpy.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


References
-
- McKenna WJ, Thiene G, Nava A, et al. Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Task Force of the Working Group Myocardial and Pericardial Disease of the European Society of Cardiology and of the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology. Br Heart J 1994;71:215–8. - PMC - PubMed
-
- Marcus FI, Fontaine GH, Guiraudon G, et al. Right ventricular dysplasia: a report of 24 adult cases. Circulation 1982;65:384–98. - PubMed
-
- Richardson P, McKenna W, Bristow M, et al. Report of the 1995 World Health Organisation/International Society and Federation of Cardiology task force on the definition and classification of cardiomyopathies. Circulation 1996;93:841–2. - PubMed
-
- Daubert JC, Descaves C, Foulgoc JL, et al. Critical analysis of cineangiographic criteria for diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Arch Mal Coeur 1991;84:33–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
