

Estimating clinical severity of COVID-19 from the transmission dynamics in Wuhan, China
- PMID: 32284616
- PMCID: PMC7094929
- DOI: 10.1038/s41591-020-0822-7
Estimating clinical severity of COVID-19 from the transmission dynamics in Wuhan, China
Erratum in
-
Addendum: Estimating clinical severity of COVID-19 from the transmission dynamics in Wuhan, China.Nat Med. 2020 Jul;26(7):1149-1150. doi: 10.1038/s41591-020-0920-6. Nat Med. 2020. PMID: 32661399 Free PMC article. No abstract available.
Abstract
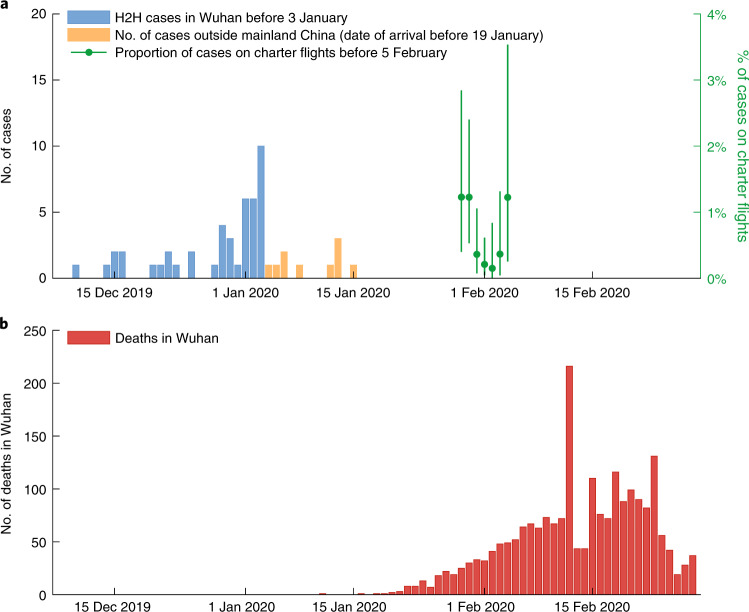
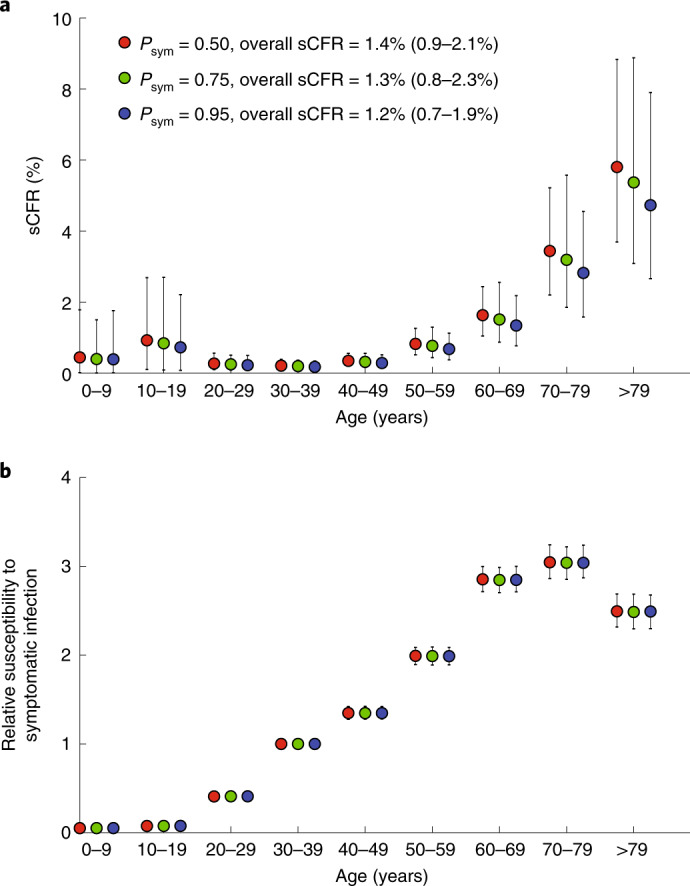
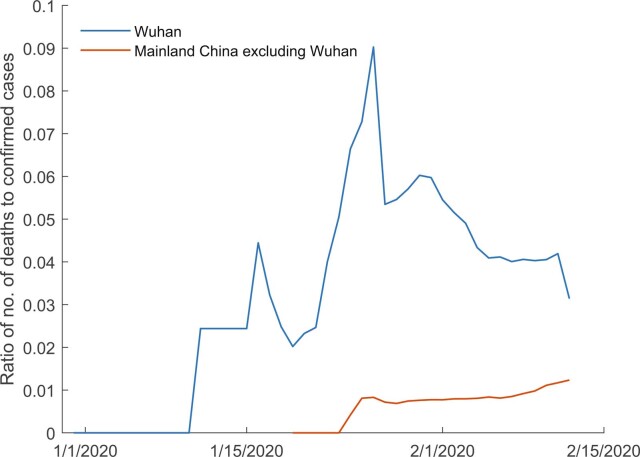
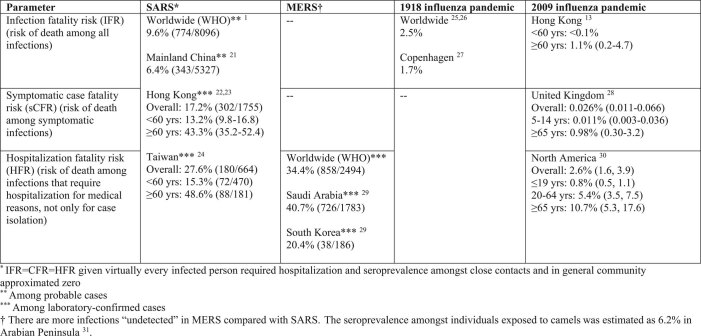
As of 29 February 2020 there were 79,394 confirmed cases and 2,838 deaths from COVID-19 in mainland China. Of these, 48,557 cases and 2,169 deaths occurred in the epicenter, Wuhan. A key public health priority during the emergence of a novel pathogen is estimating clinical severity, which requires properly adjusting for the case ascertainment rate and the delay between symptoms onset and death. Using public and published information, we estimate that the overall symptomatic case fatality risk (the probability of dying after developing symptoms) of COVID-19 in Wuhan was 1.4% (0.9-2.1%), which is substantially lower than both the corresponding crude or naïve confirmed case fatality risk (2,169/48,557 = 4.5%) and the approximator1 of deaths/deaths + recoveries (2,169/2,169 + 17,572 = 11%) as of 29 February 2020. Compared to those aged 30-59 years, those aged below 30 and above 59 years were 0.6 (0.3-1.1) and 5.1 (4.2-6.1) times more likely to die after developing symptoms. The risk of symptomatic infection increased with age (for example, at ~4% per year among adults aged 30-60 years).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
