

There are isoheight points that measure constant femoral condyle heights along the knee flexion path
- PMID: 32285156
- PMCID: PMC7554141
- DOI: 10.1007/s00167-020-05990-x
There are isoheight points that measure constant femoral condyle heights along the knee flexion path
Abstract
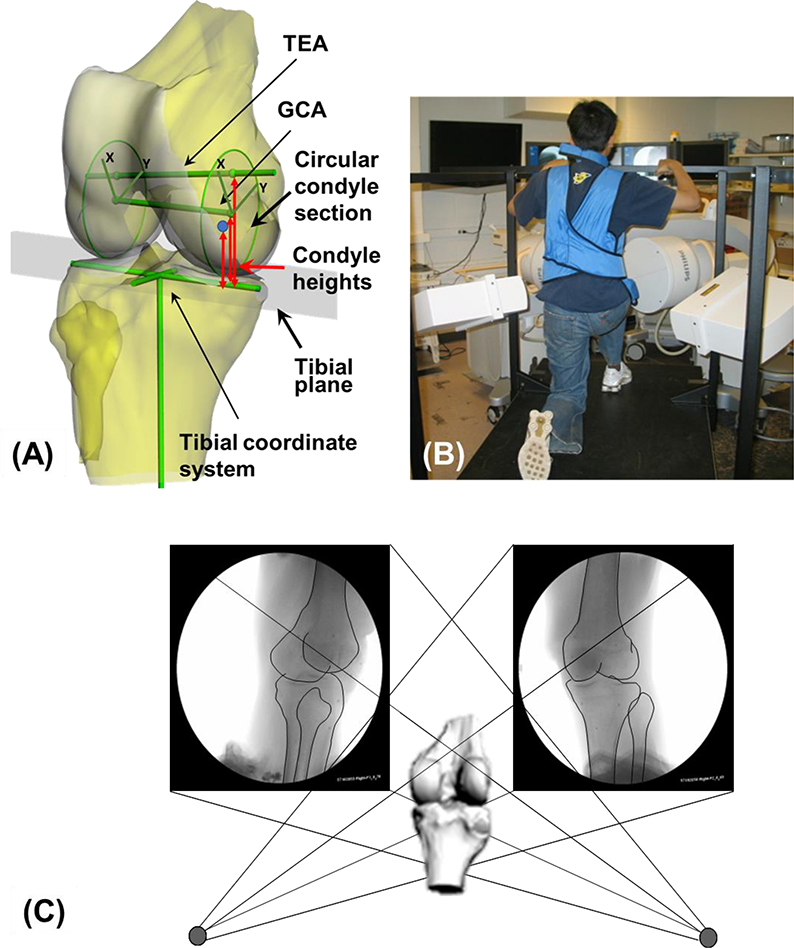
Purpose: It is a challenge to evaluate the maintenance of medial and lateral soft tissue balance in total knee arthroplasty (TKA). This study aimed to determine the "isoheight" points and the "isoheight" axis (IHA) that can measure constant medial/lateral condyle heights during flexion of the knee, and compare the IHA with two major anatomical axes, the transepicondylar axis (TEA) and the geometric center axis (GCA).
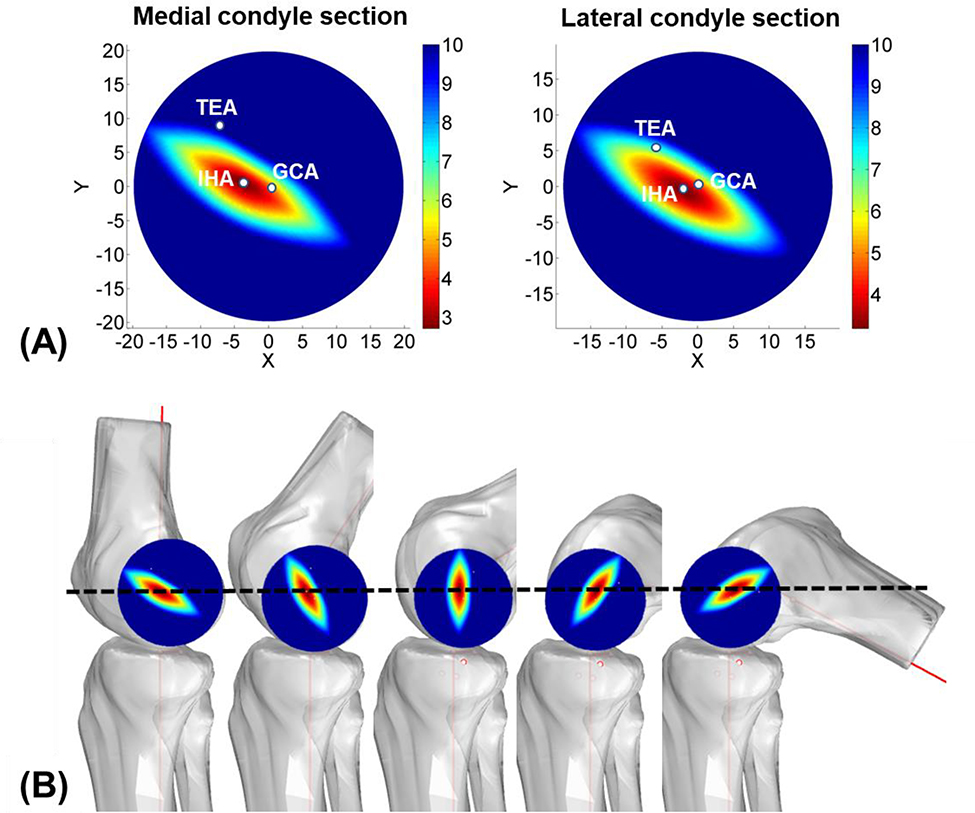
Methods: Twenty-two healthy human knees were imaged using a combined MRI and dual fluoroscopic imaging system while performing a single-legged lunge (0°-120°). The isoheight points of the medial and lateral femoral condyles were defined as the locations with the least amount of changes in heights during the knee flexion; an IHA is the line connecting the medial and lateral isoheight points. The measured changes of the condyle heights using the IHA were compared with those measured using the TEA and GCA.
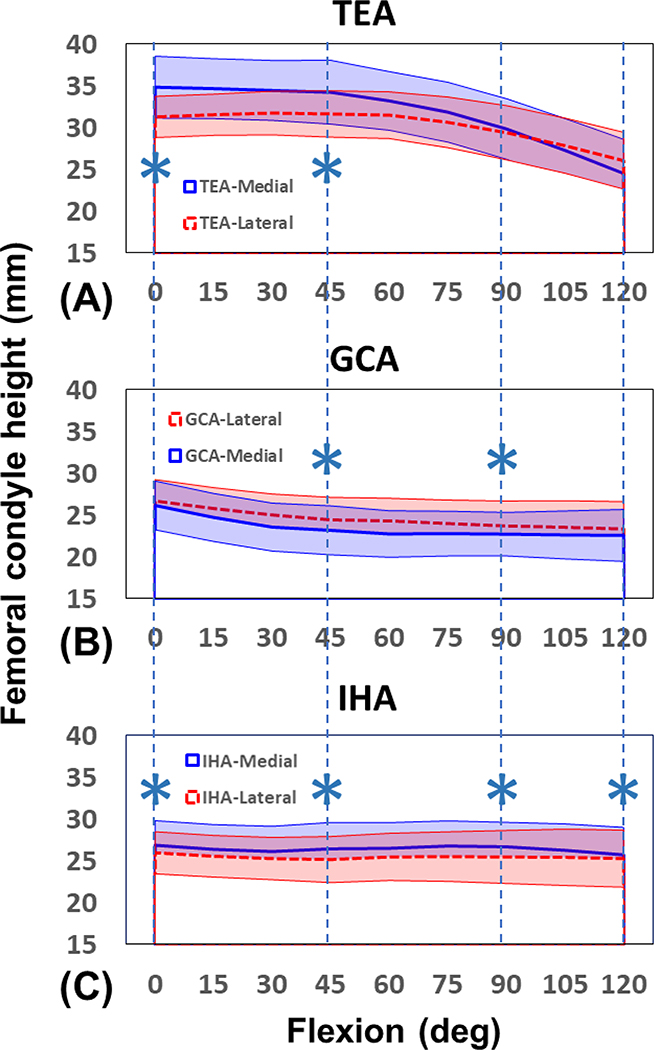
Results: Overall, the IHA was posterior and distal to the TEA, and anterior to the GCA. The isoheight points measured condyle height changes within 1.2 ± 2.3 mm at the medial and 0.7 ± 3.3 mm at the lateral sides during the knee flexion. Between 0° and 45°, the condyle height changes measured using the GCA (medial: 3.0 ± 1.8 mm, lateral: 2.3 ± 2.0 mm) were significantly larger than those of the IHA and the TEA (p < 0.05). Between 90° and 120°, the changes of the condyle heights measured using the TEA (medial: 5.3 ± 1.8 mm, lateral: 3.3 ± 1.8 mm) were significantly larger than those of the IHA and GCA (p < 0.05).
Conclusion: There are isoheight points in the medial and lateral femoral condyles that can measure constant heights along the full range of knee flexion and could be used to formulate an "isoheight" axis (IHA) of the femur. The condyle height changes measured by the TEA and GCA were greater than the IHA measurements along the flexion path. These data could be used as a valuable reference to evaluate the condyle height changes after TKA surgeries and help achieve soft tissue balance and optimal knee kinematics along the flexion path.
Level of evidence: IV.
Keywords: Femoral condyle heights; Gap balance; In vivo knee flexion; Isoheight characteristics; Soft tissue balance; Total knee arthroplasty.
Conflict of interest statement
Conflict of Interest
The authors declare that there is no conflict of interest.
Figures
References
-
- Berger RA, Rubash HE, Seel MJ, Thompson WH, Crossett LS (1993) Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis. Clin Orthop Relat Res 40–47 - PubMed
-
- Bonnin MP, Saffarini M, Bossard N, Dantony E, Victor J (2016) Morphometric analysis of the distal femur in total knee arthroplasty and native knees. Bone Joint J 98-B:49–57 - PubMed
-
- Churchill DL, Incavo SJ, Johnson CC, Beynnon BD (1998) The transepicondylar axis approximates the optimal flexion axis of the knee. Clin Orthop Relat Res 111–118 - PubMed
-
- Colle F, Bignozzi S, Lopomo N, Zaffagnini S, Sun L, Marcacci M (2012) Knee functional flexion axis in osteoarthritic patients: comparison in vivo with transepicondylar axis using a navigation system. Knee Surg Sports Traumatol Arthrosc 20:552–558 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
