

Optimizing Hydroxychloroquine Dosing for Patients With COVID-19: An Integrative Modeling Approach for Effective Drug Repurposing
- PMID: 32285930
- PMCID: PMC7262072
- DOI: 10.1002/cpt.1856
Optimizing Hydroxychloroquine Dosing for Patients With COVID-19: An Integrative Modeling Approach for Effective Drug Repurposing
Erratum in
-
Correction to "Optimizing Hydroxychloroquine Dosing for Patients With COVID-19: An Integrative Modeling Approach for Effective Drug Repurposing".Clin Pharmacol Ther. 2025 Sep;118(3):744-745. doi: 10.1002/cpt.3755. Epub 2025 Jun 29. Clin Pharmacol Ther. 2025. PMID: 40583355 No abstract available.
Abstract
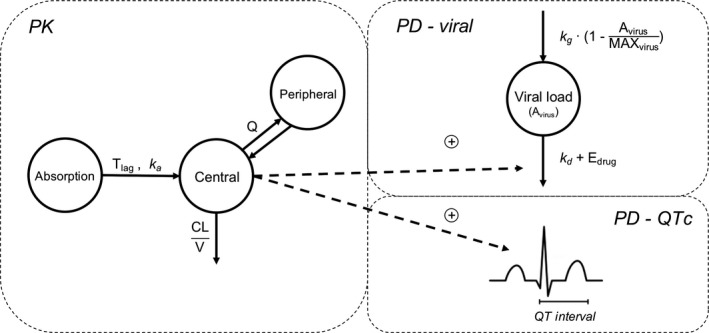
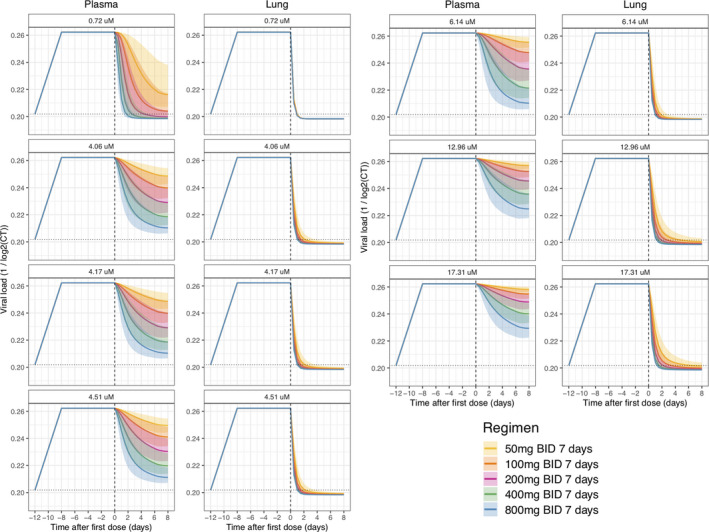
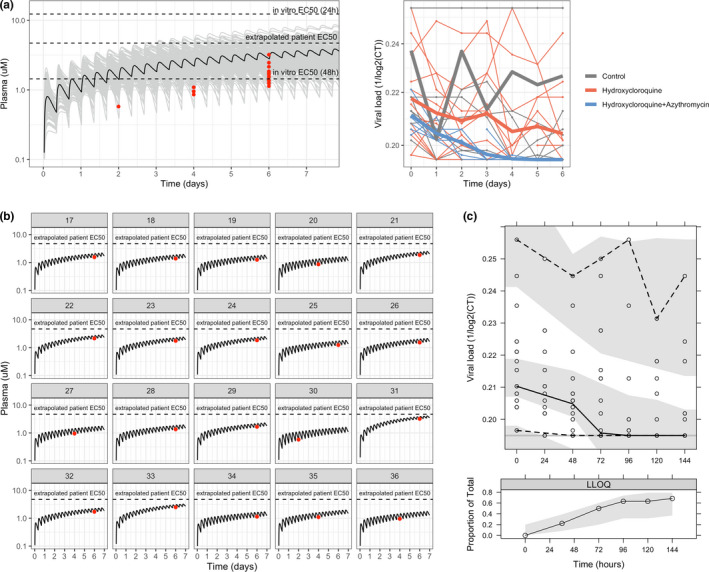
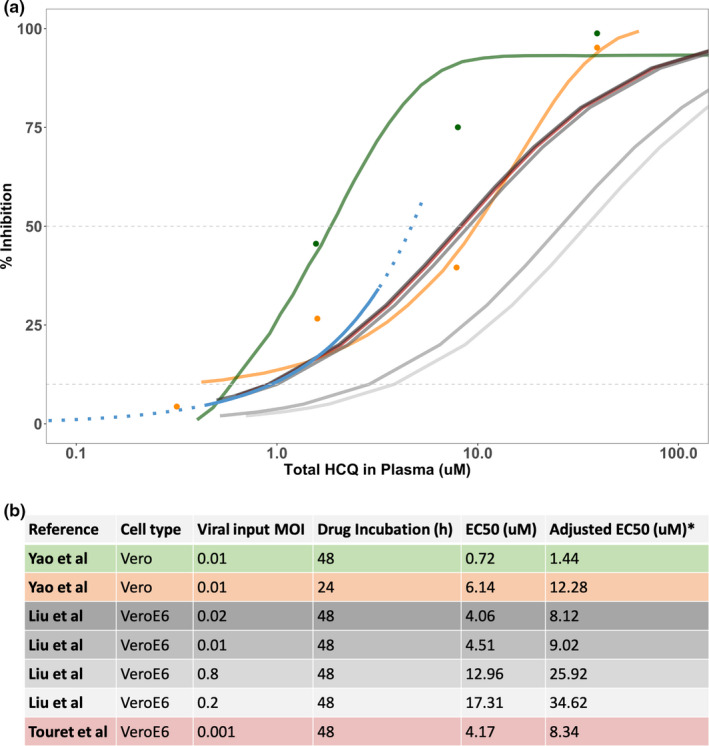
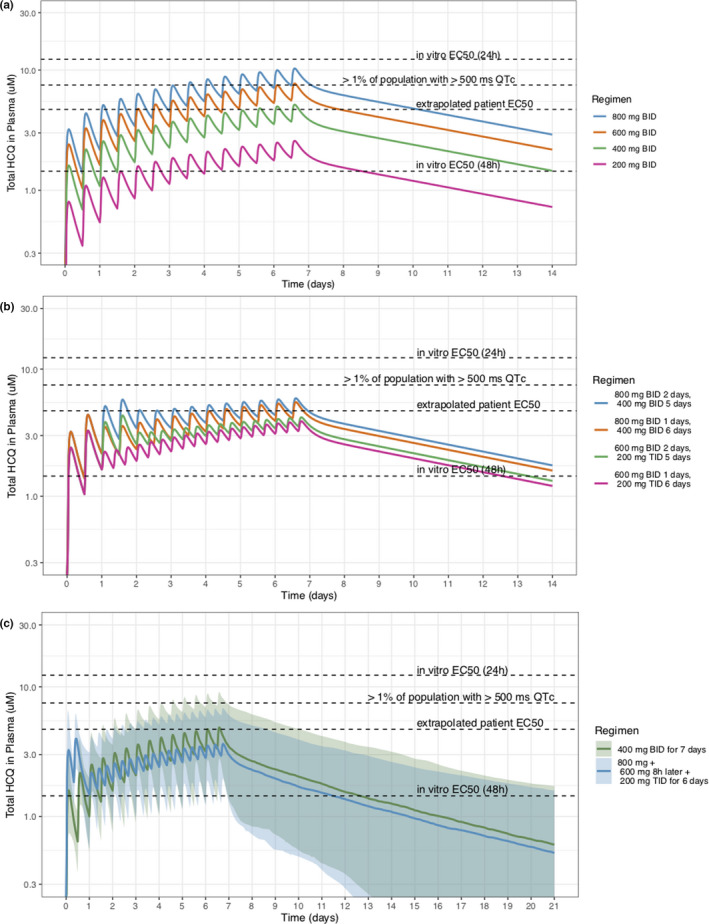
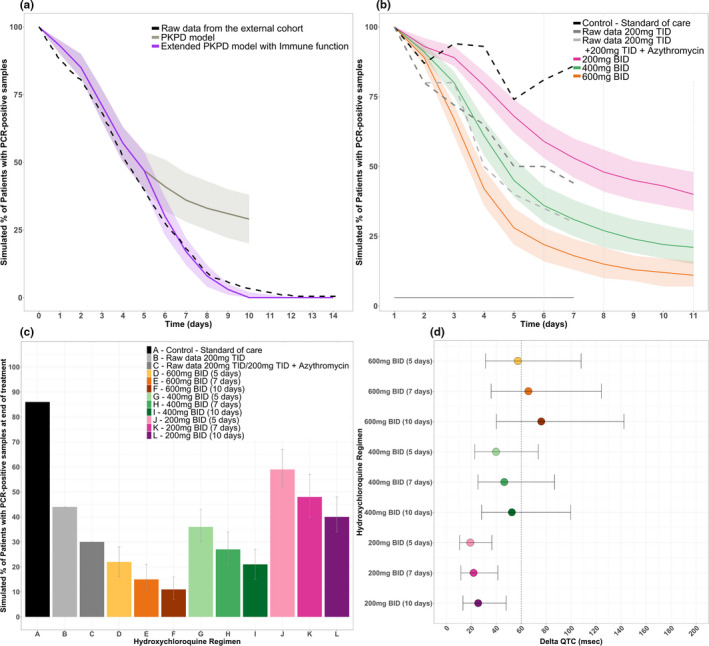
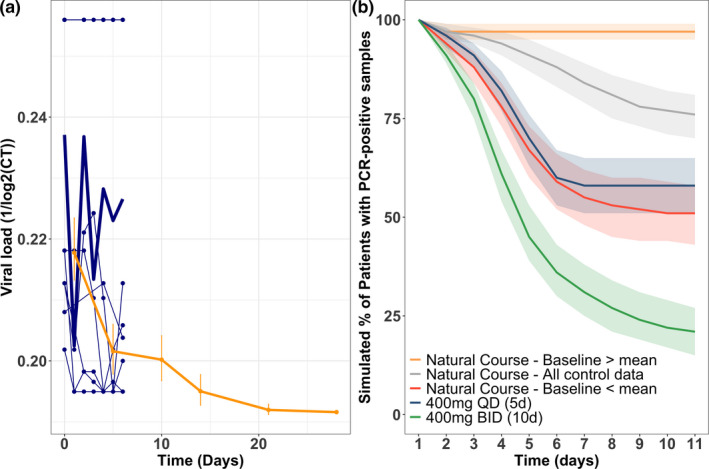
Hydroxychloroquine (HCQ) is a promising candidate for Coronavirus disease of 2019 (COVID-19) treatment. The optimal dosing of HCQ is unknown. Our goal was to integrate historic and emerging pharmacological and toxicity data to understand safe and efficacious HCQ dosing strategies for COVID-19 treatment. The data sources included were (i) longitudinal clinical, pharmacokinetic (PK), and virologic data from patients with severe acute respiratory syndrome-2 (SARS-CoV-2) infection who received HCQ with or without azithromycin (n = 116), (ii) in vitro viral replication data and SARS-CoV-2 viral load inhibition by HCQ, (iii) a population PK model of HCQ, and (iv) a model relating chloroquine PKs to corrected QT (QTc) prolongation. A mechanistic PK/virologic/QTc model for HCQ was developed and externally validated to predict SARS-CoV-2 rate of viral decline and QTc prolongation. SARS-CoV-2 viral decline was associated with HCQ PKs (P < 0.001). The extrapolated patient half-maximal effective concentration (EC50 ) was 4.7 µM, comparable to the reported in vitro EC50s . HCQ doses > 400 mg b.i.d. for ≥5 days were predicted to rapidly decrease viral loads, reduce the proportion of patients with detectable SARS-CoV-2 infection, and shorten treatment courses, compared with lower dose (≤ 400 mg daily) regimens. However, HCQ doses > 600 mg b.i.d. were also predicted to prolong QTc intervals. This prolongation may have clinical implications warranting further safety assessment. Due to COVID-19's variable natural history, lower dose HCQ regimens may be indistinguishable from controls. Evaluation of higher HCQ doses is needed to ensure adequate safety and efficacy.
© 2020 The Authors. Clinical Pharmacology & Therapeutics published by Wiley Periodicals LLC on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
The authors declared no conflict of interest.
Figures
Comment in
-
Quantitative Clinical Pharmacology Input to SARS-CoV-2 Therapeutics Should Be Based on Robust Data.Clin Pharmacol Ther. 2020 Aug;108(2):187. doi: 10.1002/cpt.1872. Epub 2020 May 20. Clin Pharmacol Ther. 2020. PMID: 32348551 Free PMC article. No abstract available.
References
-
- World Health Organization . (2020). Coronavirus disease (COVID‐19) outbreak situation <https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019> (Geneva, Switzerland,2020).
-
- Biot, C. et al. Design and synthesis of hydroxyferroquine derivatives with antimalarial and antiviral activities. J. Med. Chem. 49, 2845–2849 (2006). - PubMed
-
- Schrezenmeier, E. & Dorner, T. Mechanisms of action of hydroxychloroquine and chloroquine: implications for rheumatology. Nat. Rev. Rheumatol. 16, 155–166 (2020). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
