

First interchromosomal insertion in a patient with cerebral and spinal cavernous malformations
- PMID: 32286434
- PMCID: PMC7156631
- DOI: 10.1038/s41598-020-63337-5
First interchromosomal insertion in a patient with cerebral and spinal cavernous malformations
Abstract
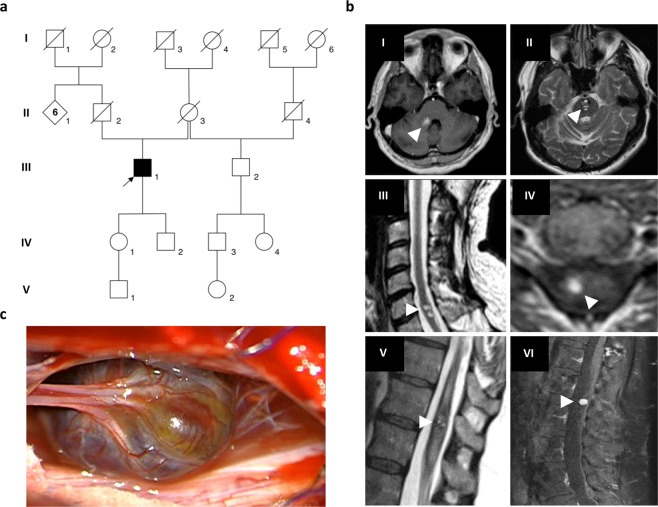
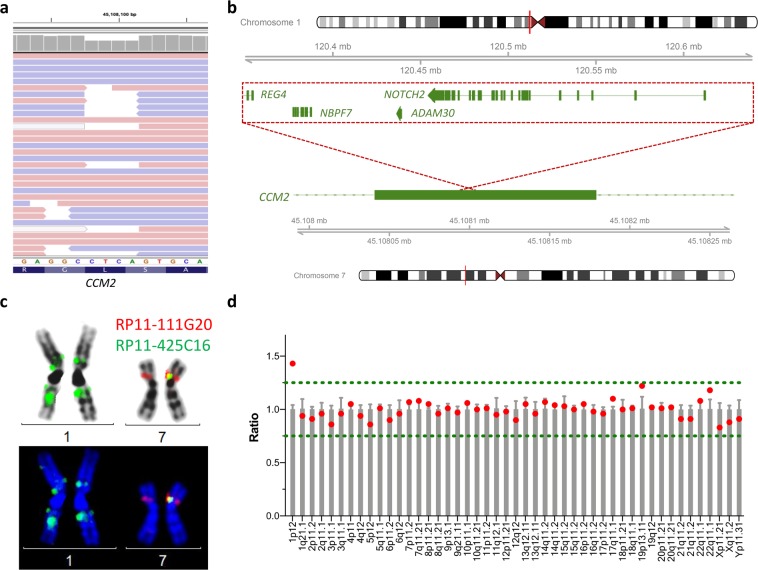
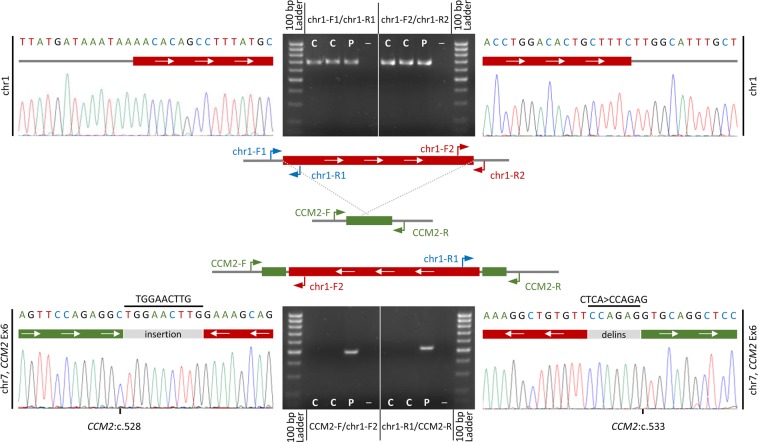
Autosomal dominant cerebral cavernous malformations (CCM) are leaky vascular lesions that can cause epileptic seizures and stroke-like symptoms. Germline mutations in either CCM1, CCM2 or CCM3 are found in the majority of patients with multiple CCMs or a positive family history. Recently, the first copy number neutral inversion in CCM2 has been identified by whole genome sequencing in an apparently mutation-negative CCM family. We here asked the question whether further structural genomic rearrangements can be detected within NGS gene panel data of unsolved CCM cases. Hybrid capture NGS data of eight index patients without a pathogenic single nucleotide, indel or copy number variant were analyzed using two bioinformatics pipelines. In a 58-year-old male with multiple CCMs in his brain and spinal cord, we identified a 294 kb insertion within the coding sequence of CCM2. Fine mapping of the breakpoints, molecular cytogenetic studies, and multiplex ligation-dependent probe amplification verified that the structural variation was an inverted unbalanced insertion that originated from 1p12-p11.2. As this rearrangement disrupts exon 6 of CCM2 on 7p13, it was classified as pathogenic. Our study demonstrates that efforts to detect structural variations in known disease genes increase the diagnostic sensitivity of genetic analyses for well-defined Mendelian disorders.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
