

Integrated Molecular and Clinical Analysis of 1,000 Pediatric Low-Grade Gliomas
- PMID: 32289278
- PMCID: PMC7169997
- DOI: 10.1016/j.ccell.2020.03.011
Integrated Molecular and Clinical Analysis of 1,000 Pediatric Low-Grade Gliomas
Abstract
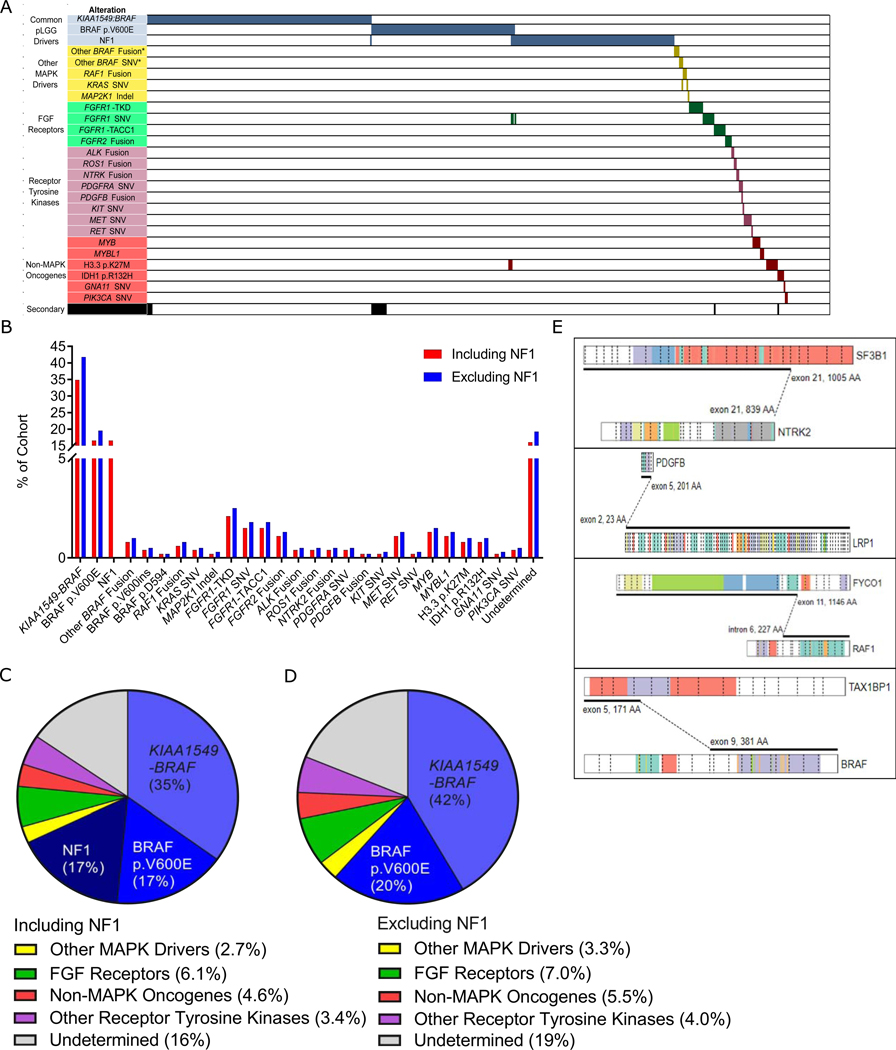
Pediatric low-grade gliomas (pLGG) are frequently driven by genetic alterations in the RAS-mitogen-activated protein kinase (RAS/MAPK) pathway yet show unexplained variability in their clinical outcome. To address this, we characterized a cohort of >1,000 clinically annotated pLGG. Eighty-four percent of cases harbored a driver alteration, while those without an identified alteration also often exhibited upregulation of the RAS/MAPK pathway. pLGG could be broadly classified based on their alteration type. Rearrangement-driven tumors were diagnosed at a younger age, enriched for WHO grade I histology, infrequently progressed, and rarely resulted in death as compared with SNV-driven tumors. Further sub-classification of clinical-molecular correlates stratified pLGG into risk categories. These data highlight the biological and clinical differences between pLGG subtypes and opens avenues for future treatment refinement.
Keywords: RAS/MAPK pathway; brain tumor; low-grade glioma; molecular diagnostics; neurooncology; pediatric; risk stratification.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests The authors declare no competing interests.
Figures






Comment in
-
The "Risk" in Pediatric Low-Grade Glioma.Cancer Cell. 2020 Apr 13;37(4):424-425. doi: 10.1016/j.ccell.2020.03.020. Cancer Cell. 2020. PMID: 32289265
-
Low-grade glioma subtypes revealed.Nat Rev Clin Oncol. 2020 Jun;17(6):335. doi: 10.1038/s41571-020-0380-4. Nat Rev Clin Oncol. 2020. PMID: 32355316 No abstract available.
References
-
- Balss J1, Meyer J, Mueller W, Korshunov A, Hartmann C, von Deimling A. (2008). Analysis of the IDH1 codon 132 mutation in brain tumors. Acta Neuropathol. 116(6): 597–602. - PubMed
-
- Banerjee A, Jakacki RI, Onar-Thomas A, Wu S, Nicolai des T, Young Poussaint T, Fangusaro J, Phillips J, Perry A, Turner D, et al. (2017). A phase I trial of the MEK inhibitor selumetinib (AZD6244) in pediatric patients with recurrent or refractory low-grade glioma: a Pediatric Brain Tumor Consortium (PBTC) study. Neuro Oncol. 19(8): 1135–1144. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
