

Trauma-Associated Pulmonary Laceration in Dogs-A Cross Sectional Study of 364 Dogs
- PMID: 32290621
- PMCID: PMC7356257
- DOI: 10.3390/vetsci7020041
Trauma-Associated Pulmonary Laceration in Dogs-A Cross Sectional Study of 364 Dogs
Abstract
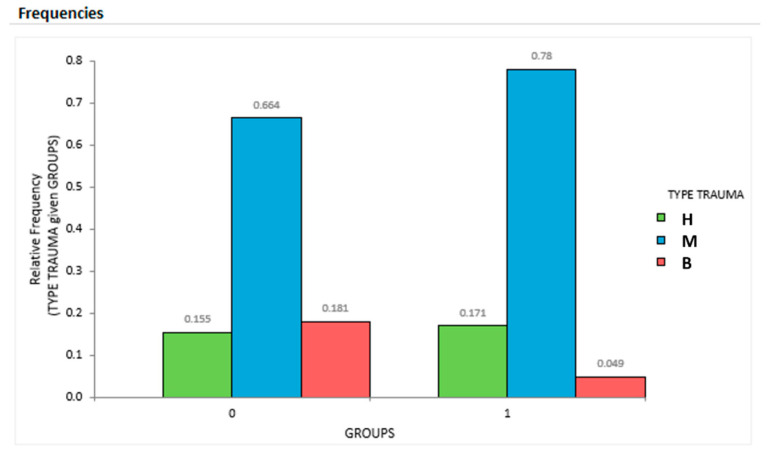
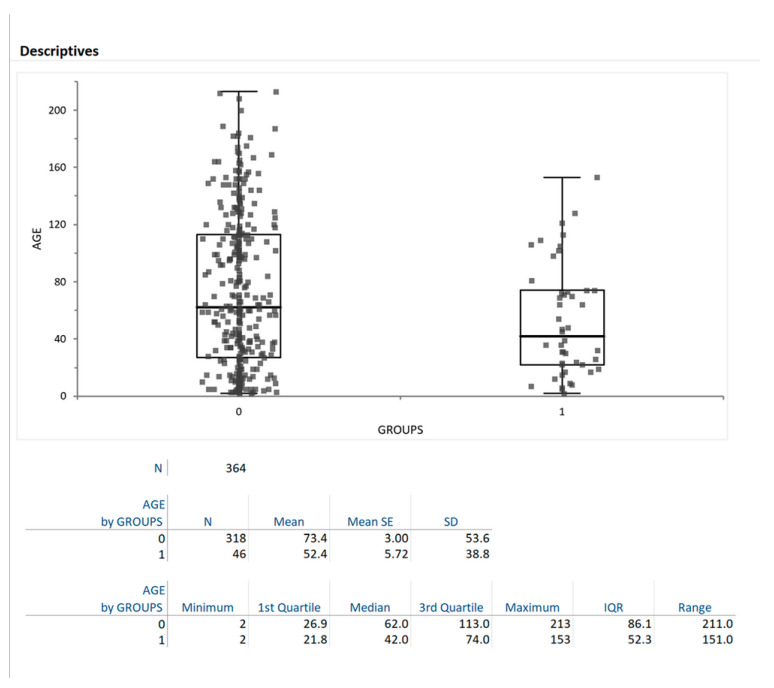
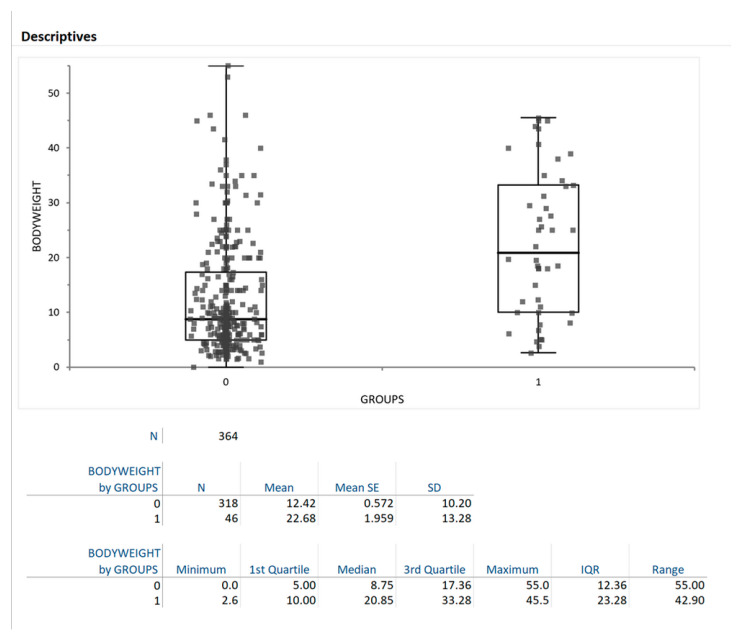
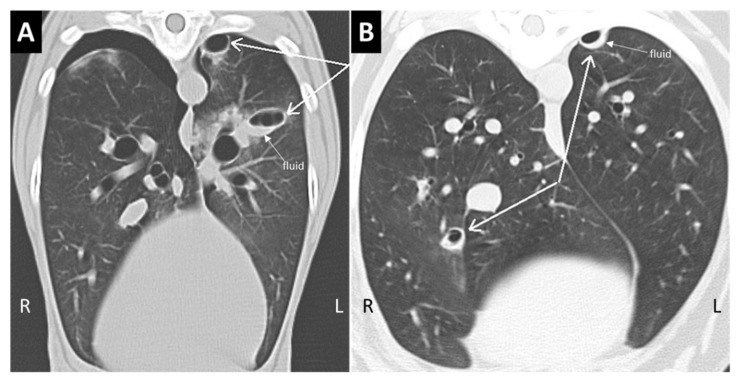
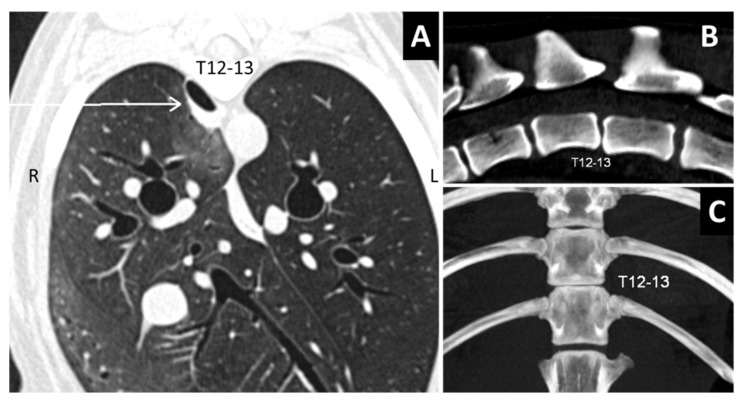
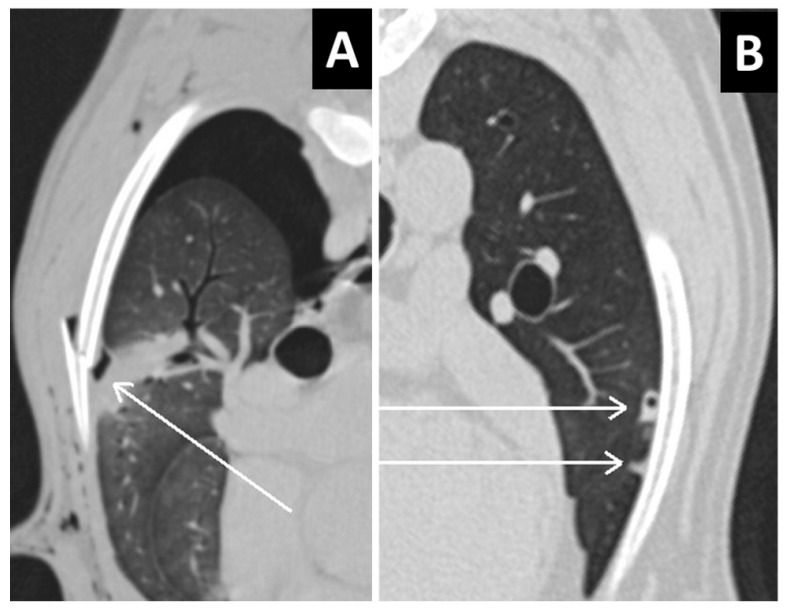
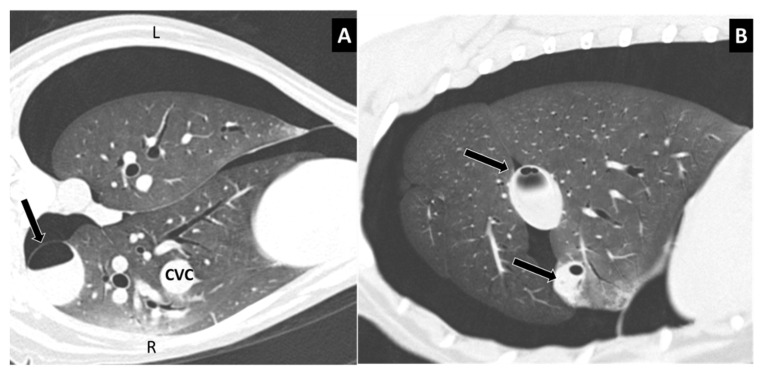
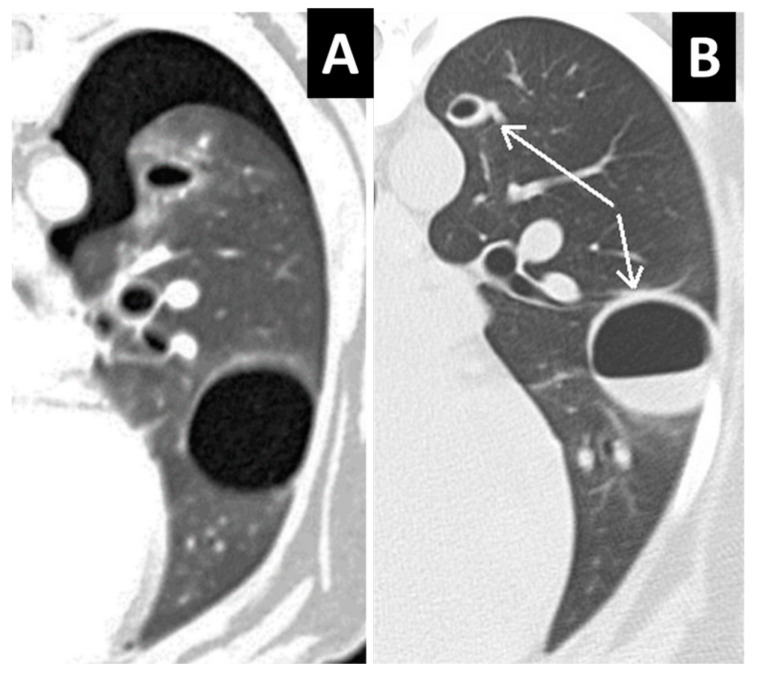
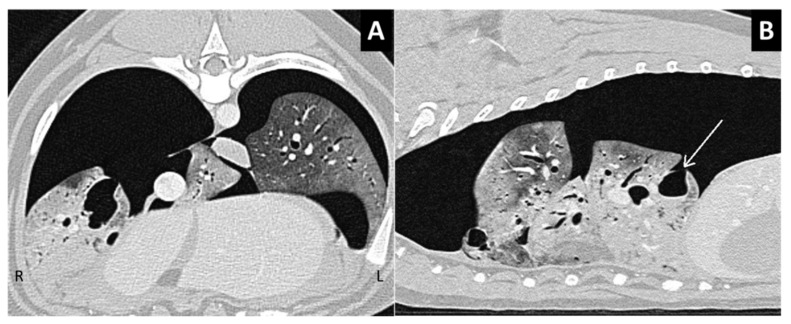
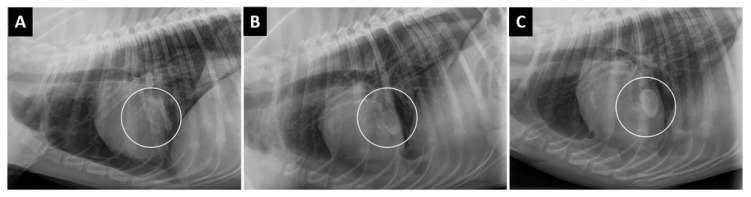
In this study, we describe the computed tomography (CT) features of pulmonary laceration in a study population, which included 364 client-owned dogs that underwent CT examination for thoracic trauma, and compared the characteristics and outcomes of dogs with and without CT evidence of pulmonary laceration. Lung laceration occurred in 46/364 dogs with thoracic trauma (prevalence 12.6%). Dogs with lung laceration were significantly younger than dogs in the control group (median 42 months (interquartile range (IQR) 52.3) and 62 months (IQR 86.1), respectively; p = 0.02). Dogs with lung laceration were significantly heavier than dogs without laceration (median 20.8 kg (IQR 23.3) and median 8.7 kg (IQR 12.4 kg), respectively p < 0.0001). When comparing groups of dogs with thoracic trauma with and without lung laceration, the frequency of high-energy motor vehicle accident trauma was more elevated in dogs with lung laceration than in the control group. No significant differences were observed between groups regarding tge frequency and length of hospitalization and 30-day mortality. Similar to the human classification scheme, four CT patterns are described in dogs in this study: Type 1, large pulmonary laceration located deeply in the pulmonary parenchyma or around an interlobar fissure; Type 2, laceration occurring in the paraspinal lung parenchyma, not associated with vertebral fracture; Type 3, subpleural lung laceration intimately associated with an adjacent rib or vertebral fracture; Type 4, subpleural lesions not associated with rib fractures. Complications were seen in 2/46 dogs and included lung abscess and collapse.
Keywords: blunt trauma; cystic lesion; laceration running head; pulmonary laceration in dogs; thoracic CT; thoracic trauma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Spackman C.J., Caywood D.D., Feeney D.A., Johnston G.R. Thoracic wall and pulmonary trauma in dogs sustaining fractures as a result of motor vehicle accidents. J. Am. Vet. Med. Assoc. 1984;185:975–977. - PubMed
LinkOut - more resources
Full Text Sources
