

Implantable Cardioverter-Defibrillators in Trials of Drug Therapy for Heart Failure: A Systematic Review and Meta-Analysis
- PMID: 32290732
- PMCID: PMC7428541
- DOI: 10.1161/JAHA.119.015177
Implantable Cardioverter-Defibrillators in Trials of Drug Therapy for Heart Failure: A Systematic Review and Meta-Analysis
Abstract
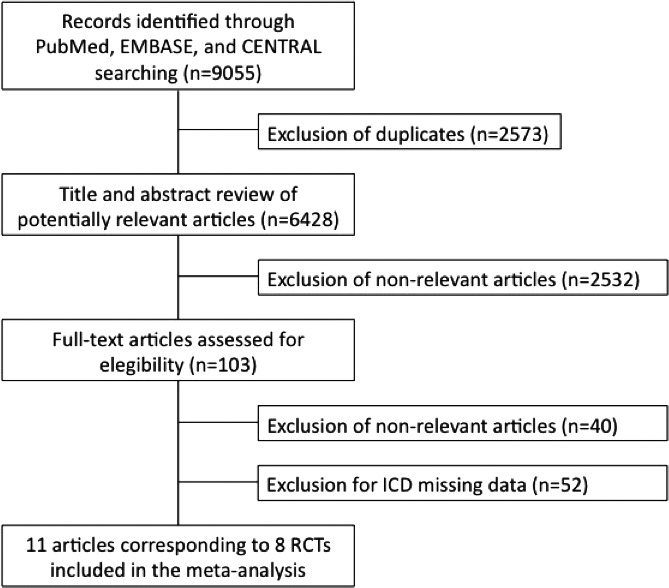
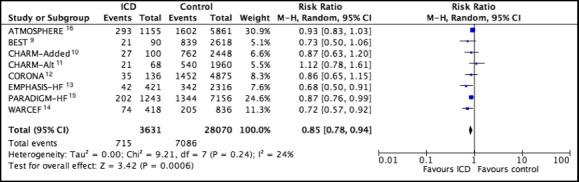
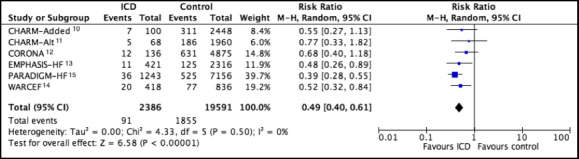
BACKGROUND Medical therapy for heart failure with reduced ejection fraction evolved since trials validated the use of implantable cardioverter-defibrillators (ICDs). We sought to evaluate the performance of ICDs in reducing mortality in the era of modern medical therapy by means of a systematic review and meta-analysis of contemporary randomized clinical trials of drug therapy for heart failure with reduced ejection fraction. METHODS AND RESULTS We systematically identified randomized clinical trials that evaluated drug therapy in patients with heart failure with reduced ejection fraction that reported mortality. Studies that enrolled <1000 patients, patients with left ventricular ejection fraction >40%, or patients in the acute phase of heart failure and study treatment with devices were excluded. We identified 8 randomized clinical trials, including 31 701 patients of whom 3631 (11.5%) had an ICD. ICDs were associated with a lower risk of all-cause mortality (relative risk [RR], 0.85; 95% CI, 0.78-0.94) and sudden cardiac death (RR, 0.49; 95% CI, 0.40-0.61). Results were consistent among studies published before and after 2010. In meta-regression analysis, the proportion of nonischemic etiology did not affect the associated benefit of ICD. CONCLUSIONS In our meta-analysis of contemporary randomized trials of drug therapy for heart failure with reduced ejection fraction, the rate of ICD use was low and associated with a decreased risk in both all-cause mortality and sudden cardiac death. This benefit was still present in trials with new medical therapy.
Keywords: all‐cause mortality; heart failure with reduced ejection fraction; implantable cardioverter–defibrillators; sudden cardiac death.
Figures
References
-
- McMurray JJV. Systolic heart failure. N Engl J Med. 2010;362:228–238. - PubMed
-
- Shen Li, Jhund PS, Petrie MC, Claggett BL, Barlera S, Cleland JGF, Dargie HJ, Granger CB, Kjekshus J, Køber L, et al. Declining risk of sudden death in heart failure. N Engl J Med. 2017;377:41–51. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, et al. Amiodarone or an implantable cardioverter–defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–237. - PubMed
-
- Shun‐Shin MJ, Zheng SL, Cole GD, Howard JP, Whinnett ZI, Francis DP. Implantable cardioverter defibrillators for primary prevention of death in left ventricular dysfunction with and without ischaemic heart disease: a meta‐analysis of 8567 patients in the 11 trials. Eur Heart J. 2017;38:1738–1748. - PMC - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;128:e240–e327. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
