

Imaging algorithm and multimodality evaluation of spinal osteoblastoma
- PMID: 32290828
- PMCID: PMC7158089
- DOI: 10.1186/s12891-020-03252-y
Imaging algorithm and multimodality evaluation of spinal osteoblastoma
Abstract
Background: To analyze the features of CT, MRI and PET/CT and their diagnostic value for spinal osteoblastomas (OBs).
Methods: The radiological and clinical data of 21 patients with histopathologically-confirmed spinal OBs were analyzed retrospectively.
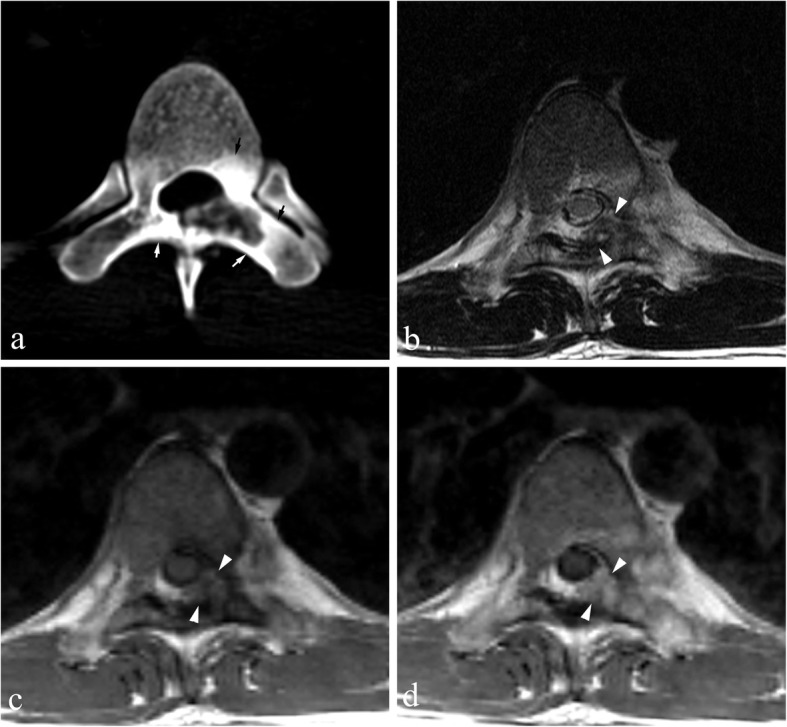
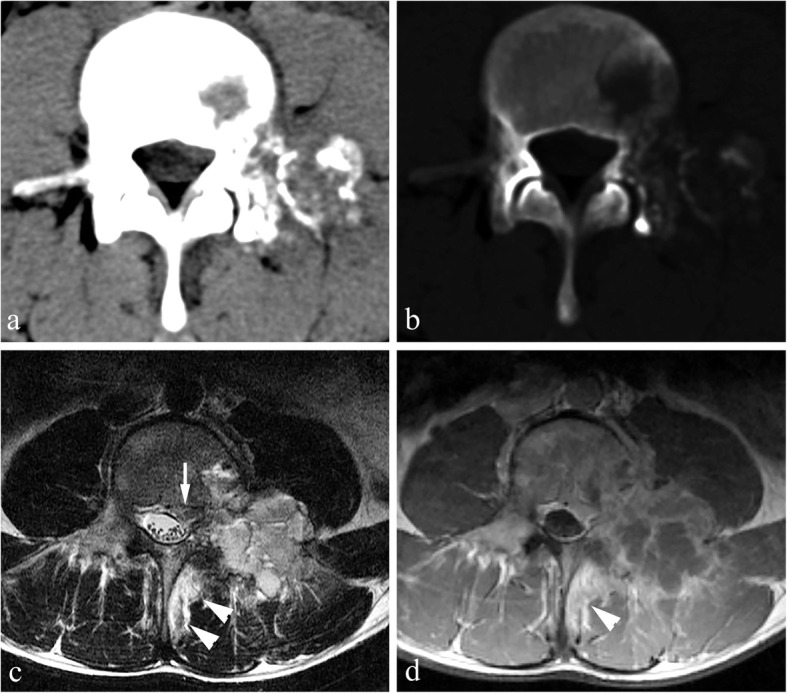
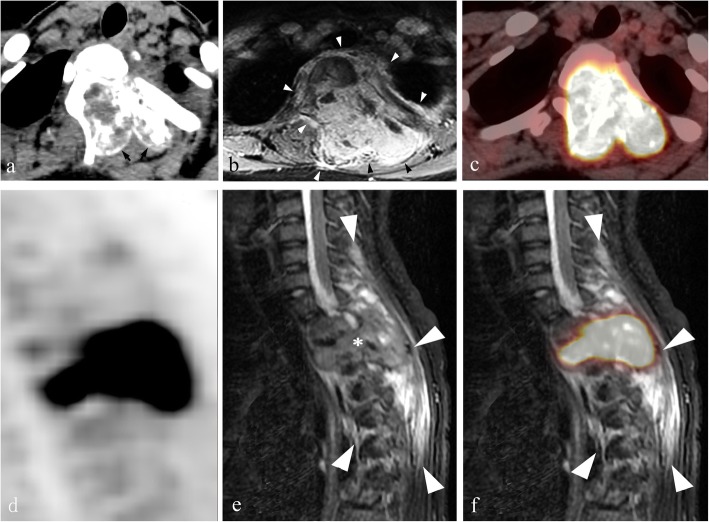
Results: Sixteen of the 21 cases were benign and 5 were aggressive OBs. Tumors were located in the lumbar (n = 11), cervical (n = 4), thoracic (n = 5), and sacral (n = 1) spinal regions. Nineteen cases were centered in the posterior elements of the spine, 13 of which extended into the vertebral body. Punctate or nodular calcifications were found in all cases on CT with a complete sclerotic rim (n = 12) or incomplete sclerotic rim (n = 8). The flare phenomenon (indicative of surrounding tissue inflammation) was found in 17/21 cases on CT, thin in 11 cases and thick in 6 cases, and in 19/19 cases on MRI, thin in 1 case and thick in 18 cases. On 18F-FDG PET/CT, all cases (8/8) were metabolically active with the SUVmax of 12.3-16.0; the flare sign was observed in 8 cases, including 7 cases of hypometabolism and 1 case of coexistence of hypermetabolism and hypometabolism. Based on CT, 3, 12, and 6 cases were classified as Enneking stage 1, 2 and 3, respectively. Of 19 cases with MRI, 1 and 18 cases were classified as Enneking stage 2 and 3, respectively.
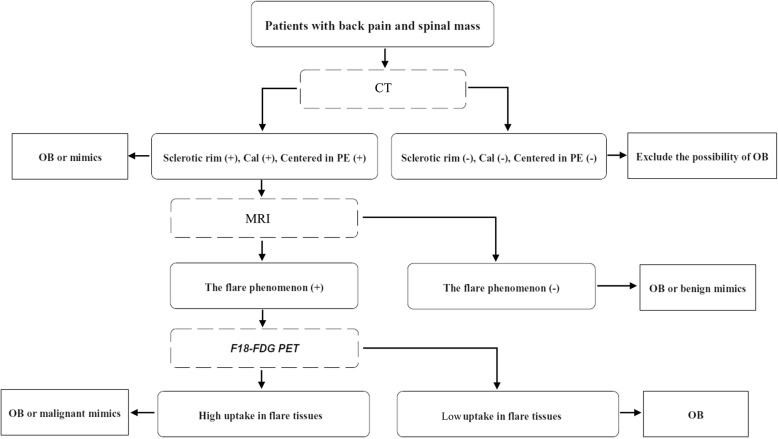
Conclusions: Spinal OB has multiple unique characteristic radiological features. Although a larger sample size is needed, combining CT, MRI and PET may be beneficial to optimize preoperative diagnosis and care of patients with OBs.
Keywords: CT, MRI, PET; Osteoblastoma; Radiography; Spine.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Tang H, Zou D, Chen W. Imaging diagnosis of aggressive osteoblastoma. J Clin Radiol. 2011;30:76–78.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
